Business Wire05.15.17
Shockwave Medical, a pioneer in the treatment of calcified cardiovascular disease, announced conformité européenne (CE) Mark for the company’s Coronary Lithoplasty System for the treatment of calcified plaque in conjunction with stenting in patients with coronary artery disease.
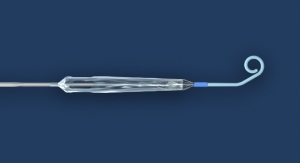
The Shockwave Medical Coronary Lithoplasty System is an innovative therapy designed to treat calcified coronary artery blockages with lithotripsy, sonic pressure waves historically used to treat patients with kidney stones.
The presence of calcified coronary artery disease leads to suboptimal outcomes for all treatment options—medical therapy, interventional treatment and cardiac surgery.1 For angioplasty with a stent, the presence of calcified lesions is associated with suboptimal lesion expansion, poor stent apposition and complications including dissection, distal embolization, coronary hypoperfusion and procedural failure.2 Specialty balloons and atherectomy are current adjunctive therapies designed to modify coronary calcium. Their use is limited due to risk of complications, degree of technical difficulty, operator dependency or lack of sufficient evidence.1,3
“Cardiovascular calcification presents a persistent treatment challenge for the interventionalist,” said Jean Fajadet, M.D., co-director of the Interventional Cardiovascular Group at Clinique Pasteur in Toulouse, France, and co-principal investigator of the DISRUPT CAD I clinical trial of the technology. “The use of Lithoplasty in the coronary arteries is an important new option that has shown, in the DISRUPT CAD I clinical study of the device, to effectively prepare the vessel for stent implantation with minimal complications. I look forward to commercial availability of the system.”
Safety and performance was supported by clinical data from results of DISRUPT CAD I, a pre-market, prospective multi-center single-arm study conducted at seven centers in Europe and Australia. The study evaluated the use of the Shockwave Medical Coronary Lithoplasty System as a treatment for calcified coronary arteries prior to drug eluting stent (DES) implantation. Primary endpoint results from the study were reported last fall at the annual Transcatheter Cardiovascular Therapeutics (TCT) conference in Washington, D.C.
“CE Mark for the Coronary Lithoplasty System is an important milestone for Shockwave Medical,” said Shockwave Medical CEO Doug Godshall. “With this achievement, we are a step closer to bringing Lithoplasty to patients and physicians in Europe as a potentially paradigm-changing technology for the treatment of coronary artery disease. We look forward to sharing our final six-month results from DISRUPT CAD I at EuroPCR this week, and to continuing to gather clinical evidence on the benefits of this promising treatment for a challenging patient population.”
References
1Madhavan M, Généreux P, et al. Coronary Artery Calcification: Pathogenesis and Prognostic Implications. J Am Coll Cardiol 2014;63:1703–14.
2Lee M, Shah N. The Impact and Pathophysiologic Consequences of Coronary Artery Calcium Deposition in Percutaneous Coronary Interventions. J Invasive Cardiol 2016;28(4):160-167.
3Tomey M, Kini A, Sharma S. Current Status of Rotational Atherectomy. J Am Coll Cardiol Intv 2014;7:345–53.
The Shockwave Medical Coronary Lithoplasty System is an innovative therapy designed to treat calcified coronary artery blockages with lithotripsy, sonic pressure waves historically used to treat patients with kidney stones.
The presence of calcified coronary artery disease leads to suboptimal outcomes for all treatment options—medical therapy, interventional treatment and cardiac surgery.1 For angioplasty with a stent, the presence of calcified lesions is associated with suboptimal lesion expansion, poor stent apposition and complications including dissection, distal embolization, coronary hypoperfusion and procedural failure.2 Specialty balloons and atherectomy are current adjunctive therapies designed to modify coronary calcium. Their use is limited due to risk of complications, degree of technical difficulty, operator dependency or lack of sufficient evidence.1,3
“Cardiovascular calcification presents a persistent treatment challenge for the interventionalist,” said Jean Fajadet, M.D., co-director of the Interventional Cardiovascular Group at Clinique Pasteur in Toulouse, France, and co-principal investigator of the DISRUPT CAD I clinical trial of the technology. “The use of Lithoplasty in the coronary arteries is an important new option that has shown, in the DISRUPT CAD I clinical study of the device, to effectively prepare the vessel for stent implantation with minimal complications. I look forward to commercial availability of the system.”
Safety and performance was supported by clinical data from results of DISRUPT CAD I, a pre-market, prospective multi-center single-arm study conducted at seven centers in Europe and Australia. The study evaluated the use of the Shockwave Medical Coronary Lithoplasty System as a treatment for calcified coronary arteries prior to drug eluting stent (DES) implantation. Primary endpoint results from the study were reported last fall at the annual Transcatheter Cardiovascular Therapeutics (TCT) conference in Washington, D.C.
“CE Mark for the Coronary Lithoplasty System is an important milestone for Shockwave Medical,” said Shockwave Medical CEO Doug Godshall. “With this achievement, we are a step closer to bringing Lithoplasty to patients and physicians in Europe as a potentially paradigm-changing technology for the treatment of coronary artery disease. We look forward to sharing our final six-month results from DISRUPT CAD I at EuroPCR this week, and to continuing to gather clinical evidence on the benefits of this promising treatment for a challenging patient population.”
References
1Madhavan M, Généreux P, et al. Coronary Artery Calcification: Pathogenesis and Prognostic Implications. J Am Coll Cardiol 2014;63:1703–14.
2Lee M, Shah N. The Impact and Pathophysiologic Consequences of Coronary Artery Calcium Deposition in Percutaneous Coronary Interventions. J Invasive Cardiol 2016;28(4):160-167.
3Tomey M, Kini A, Sharma S. Current Status of Rotational Atherectomy. J Am Coll Cardiol Intv 2014;7:345–53.