|
Yoshio Mitsumori |
The broad outline for a healthcare reform plan was authorized as of November 30, 2005. Several medical reform summit meetings, hosted last November by Prime Minister Junichiro Koizumi and attended by the Minister of Finance, Minister of Health, Labor & Welfare, Cabinet Secretary General and top executives of supporting parties, have investigated this healthcare reform plan after reviewing the preliminary draft made by the Ministry of Health, Labour & Welfare (MHLW). The main points addressed included
• Direction of medical remuneration
• Improvement of quality of medicine focused on preventive measures
• Moderation of medical expenditure
• Re-examination of the health insurance program
• Restructuring of the Central Social Insurance & Medical Council (CHUIKYO)
Plan Ideology
The reform plan adheres to three basic philosophies.
First, establish a reliable healthcare system that will provide high-quality medical services, and convert the therapeutic emphasis to a focus on prevention.
Next, maintain universal insurance coverage while balancing medical expenditures with the national economy. An acceptable healthcare structure will be explored by monitoring the growth of medical expenditures with tangible indicators. Cost containment programs should be promoted for areas such as control of lifetime diseases and shorter hospital stays. Evaluate unnecessary expenditures and re-examine the scope of insurance coverage.
Finally, establish the new medical insurance system for elderly individuals and differentiate the “elderly” and “active” generations. Unify the medical insurance system by consolidating local insurance organizations on a prefecture basis.
Focus on the Elderly
The current payment structure for insured individuals will incur some changes under the new health plan. Copayments for wealthier individuals older than 70 years will increase from 20% (present rate) to 30%, beginning in October 2006. After fiscal 2008, the copayment for 70- to 74-year old individuals with low-to-moderate income will also increase from 10% to 20%. In addition, new healthcare insurance will be established for elderly individuals who are older than 75 years.
The 20% copayment for children younger than 3 years of age will also be expanded to include those “before the age of compulsory education.”
The ideology behind these types of measures is that the elderly population will assume a fair burden to help support young families with small children.
Behind the Scenes
In the decision-making process, the most powerful player was the office of the Prime Minister. MHLW and the supporting parties proposed that copayments for people in their late 60s be reduced from 30% to 20%. However, Prime Minister Koizumi flatly rejected this idea and insisted on maintaining the current percentage.
Koizumi also helped abolish the current recommendation system of CHUIKYO members, who investigate healthcare remunerations and/or cost allocation. Under the old system, powerful lobbying organizations such as the Japan Medical Association (JMA)—supported by the Diet backers—practically controlled the CHUIKYO meeting.
Of course, JMA and its supporters strongly oppose the abolishment—but Koizumi consistently brushed off the opposition. During the investigation, the Council of Economic and Fiscal Policy (CEFP)—the Prime Minister’s advisory board consisting of representatives from the private sector—also investigated the healthcare reform plan and significantly influenced the decision-making process.
Looking toward the future, huge gaps were found in the projections by MHLW and CEFP. The total medical benefit to be paid in fiscal 2006 is an estimated 28 trillion Yen (7.3% on GDP), and it will increase up to 56 trillion Yen (10.5% on GDP) by 2025 if the system remains the same. The MHLW seeks to cut the benefit expenditure to 49 trillion Yen (9.1% on GDP) by introducing its proposed reform plan, while CEFP proposes reductions to 42 trillion Yen (7.8% on GDP).
As a result, the healthcare reform plan outline incorporated a “tangible indicator” to assess the benefit expenditure every 5 years.
In general, the Japanese healthcare cost per GDP is not high in comparison with other countries. Among 30 OECD countries, Japan is ranked at 18 (see Figure 1).
A general concern remains that the deviation between the national economy and healthcare expenditure may collapse the universal healthcare coverage. However, in consideration of the growing elderly population and improving medical technology, it might be difficult to press down the medical expenditure within the scope of economy growth.
The government will present the healthcare reform bill to the Diet at the next ordinary session. Considering the current political situation, the bill should pass through the Diet without any delay.
Budget Matters
With healthcare reform matters almost settled, another consideration is the budget assessment for fiscal 2006. Attention is shifting toward the reduction of medical remuneration.
This year will encounter the biennial re-pricing for all medical service fees and drug/medical material costs. Prices for drugs and medical materials have been consistently reduced in the past, but medical service fees were only reduced once, in 2002.
If copayments are increased for patients, medical service fees inevitably will be reduced. The Ministry of Finance suggests cutting approximately 5% on the total basis, which means a reduction of about 1.5 trillion Yen by the medical service fee and drug/medical material cost.
It is not surprising that JMA and the pharmaceutical and medical device industries object strongly. MHLW and representatives from each sector will have serious negotiations down the road. Regardless, Koizumi’s strong leadership may force the significant cut.
As part of the negotiation process, CHUIKYO hosted a meeting with the medical device industry on November 18. Attendees included representatives from the Japan Federation of Medical Device Associations (JFMDA), American Chambers of Commerce of Japan (ACCJ)/Medical Device Subcommittee, AdvaMed and the European Business Community of Japan.
Each representative explained the peculiar nature of medical devices, differences with pharmaceuticals, problems on the current system and so on. Some common concerns emerged:
• Compliance with new requirements, per the regulatory amendment (as of April 2005), will force the industry to bear an additional cost about 560 billion Yen.
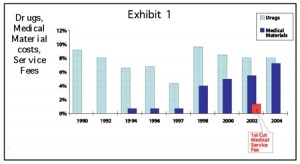
• Continuous reduction of reimbursement prices has significantly decreased the portion of medical devices per gross expenditure (see Figure 2).
• Assessment of reimbursement prices for new functional medical devices is very slow.
In addition, the industry also believes the current system’s incentives for development of new medical technology or investment do not work.
Reimbursement prices for medical materials are at the upper limit at 150% as much as FAP (foreign average price). However, the definition of FAP has not been clear between MHLW and the industry—this always seems to become a point of argument.
Nevertheless, critics believe medical materials are still too expensive in comparison with the other leading countries. Therefore, it seems inevitable that some prices will be cut for medical materials in April 2006. The industry, however, tries hard to minimize the price cut as much as possible.
Since 40% of medical devices being used in Japan are foreign-made products, the concern remains that foreign investors will deteriorate. Consequently, Japanese patients would not be able to access the latest medical technology. The high burden of compliance to the new requirements and reduced reimbursement may restrict business activities in the market. A fair and appropriate assessment is expected.
Yoshio Mitsumori is the president and CEO for Tokyo-based ADMIS, a consultant specializing in the medical device industry. He has more than 25 years of experience in the medical industry, including positions with the Itochu Corp., U.S. Surgical, National Medical Enterprises and Century Medical. A member of RAPS, he has spoken at many industry events and worked extensively in international trade of medical products and technologies. He can be reached at ymitsumori@admis.co.jp.