|
Yoshio Mitsumori |
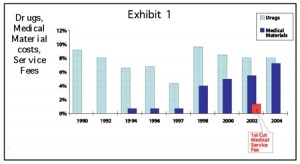
The wrangling over postal reform couldn’t have come at a worse time for the medical device industry because pension and medical reforms are also up for discussion. A reform of the Japanese medical system was originally picked up by policy makers in 2003 (Fig. 1), with the goal of drafting a basic policy by 2006 and enacting it in 2008. Despite heated exchanges over postal reform, all stakeholders have been carefully focusing on ways to make medical reform work. The key points have been on controlling ever-growing medical expenditure for the elderly and how to spread the burden among beneficiaries. Two principle measures being considered by the Ministry of Health, Labor & Welfare (MHLW) are the establishment of a new “Elderly-Care Medical Insurance System” and the restructuring of the existing healthcare insurance system.
Annual medical expenditures for patients over 75 under the current insurance system is estimated at more than $100 billion (¥11 trillion), which is about one third of total medical spending, and this will easily triple by 2035 under the existing system, which fails to motivate the elderly to cut medical spending. It is estimated that medical spending for one elderly patient is about five times the amount for younger generations.
Under the proposed reform plan, patients over 75 would join a separate insurance system and be required to share a partial burden of medical costs. This is necessary because the burden on working adults will become increasingly difficult as time goes by. The proposed system is aimed at shifting costs to designated districts. For example, the more that a district spends on the elderly, the heavier the burden on residents in that district. The goal is to promote cost savings for medical expenditure within each area. For those younger than 75, they can continue to participate in the current insurance system.
The MHLW is about to complete a draft of reform bill this autumn, submit it to reviewers and present it to the regular Diet session in the next fiscal year. The MHLW intends to establish a new elderly insurance system by fiscal 2008. However, huge gaps exist among the stakeholders such as the central government, local government, industry, labor unions and medical professionals.
The proposed plan is to limit the public burden to 50%, with the other 50% covered by the elderly and working adults. However, the ratio for the elderly and working adults has not been decided yet. The Japan Medical Association (JMA) is insisting that the public burden and support from working adults should be 80%.
Age has also become a big arguing point. The Japan Business Federation (JBF) insists that anyone under 64 should be included in the new insurance system. The MHLW proposal, however, includes those between 65 and 74 in its framework of contributing adults. Another point is co-payments. The MHLW proposes that co-payment be 10% for the general population and 20% for wealthy elderly patients. The JBF proposes 20% for outpatient and 30% for inpatient, while the JMA wants a flat rate of 10%.
Another question is who will manage and control the new insurance system— the central government or local government? As a result, many issues remain unresolved and the debate will surely heat up.
For working adults, the MHLW is planning to reduce healthcare expenditure by introducing radical preventive measures rather than through coverage reduction. Eight parameters will be set up to be indicators of health improvements in each district, including the number of check-ups, cancer examination, patient education, inpatient days, the establishment of local support mechanisms, coverage areas, home healthcare and mortality ratio. For example, if the percentage of patients who receive regular check-ups were increased from 60% to 90%, lifestyle diseases such as diabetes, hypertension and others could be prevented at an early stage. The MHLW predicts that these preventive measures may reduce the severity of illnesses by 20% and save the country ¥2.8 trillion by 2025.
Hospital stays are an important indicator in social reintegration. The average Japanese stay is 36.4 days, while in the U.S. the average is less than six days. The MHLW intends to shorten hospital stays by shifting chronic care from hospitals to secondary facilities or to the home. By adopting these eight parameters, the ministry predicts it could save ¥7.7 trillion by 2025.
“Mixed Billing”
Another change officials are embracing is expanding the “mixed billing” of medical services, which combines insured and uninsured products used in a procedure.
Traditionally, all medical services must be performed within the framework of the National Health Insurance. Uninsured medical services or devices cannot be used with insured services. Highly advanced medical technology has been the only exemption. This exception allows the hospital to charge the costs of advanced technology directly to the patient, but all other costs in a procedure would be reimbursable under insurance. The MHLW restricted advanced technology to qualified institutions with more than 300 beds, but recently it has decided to ease the restriction to facilities of all sizes. This deregulation will be effective beginning this month. Small clinics or hospitals with fewer than 300 beds can provide “mixed billing” medical services if they qualify under the other requirements such as allocation of specialty physicians, experienced paramedics and specific infrastructure.
This expansion could be a boon for new medical device manufacturers. Like the U.S., Japan requires device manufacturers to provide clinical data proving efficacy and economic benefits before reimbursement is approved. This process can be time consuming. Marketing novel devices as a highly advanced medical technology may be a good alternative solution. Even without reimbursement from insurance, institutions can charge the costs of new technology to the patient, and this may accelerate sales.
However, there is a catch: applicants seeking the highly advanced medical technology route must be the medical institution and not the manufacturer or distributor. Therefore, companies must work very closely with the institutions. Incremental improvements in a technology, however, cannot qualify as highly advanced medical technology if a similarly technology is currently reimbursable through insurance. Improved products can either be reimbursed under the existing rate, or the manufacturer must apply for new coding.
Another problem is the cost of service. Insured medical services are priced at the same rate at any hospital in Japan; however, the price of uninsured medical services is set by the hospital. This may cause some confusion in the market. For instance, in the case of a laparoscopic hepatectomy, some hospitals charge about $1,560, while others charge as much as $2,300. The difference comes from the cost of medical products used in the procedure, personnel costs, utility costs and so on.
Currently 101 types of highly advanced medical technology procedures are performed at 108 hospitals in Japan, but the price to the patient varies depending upon the hospital. Further deregulation may accelerate this trend. This is a result, of course, of deregulation, and the market will ultimately accept this disparity. This also means hospitals will be selected in accordance to its reputation, experience and associated services. That’s when the real market forces will kick in.
Yoshio Mitsumori is the president and CEO for Tokyo-based ADMIS, a consultant specializing in the medical device industry. He has more than 25 years of experience in the medical industry, including positions with the Itochu Corp., U.S. Surgical, National Medical Enterprises and Century Medical. A member of RAPS, he has spoken at many industry events and worked extensively in international trade of medical products and technologies. He can be reached at ymitsumori@admis.co.jp