Maria Shepherd, President and Founder, Medi-Vantage03.10.23
It's been approximately 20 years since value analysis committees (VACs) have become the norm in hospital purchasing, and they have become much more sophisticated. VACs were initiated to guide hospitals, ambulatory surgery centers, and other healthcare organizations to align their goals, processes, and practices to better conform to the healthcare delivery model that rewards hospitals delivering high quality care safely, efficiently, and capably, while fining those that do not deliver on these objectives. These fines, derived from reimbursement penalties, can be significant, especially for hospital systems that operate on razor-thin margins.
It's not all about reducing the price of devices. Salespeople need to be versatile in presenting the value of their products and services to the economic or clinical buyer who will likely have many nuanced questions relevant to their functional perspective. Needless to say, it's not as easy as it used to be. However, there are still three main guidelines medical device companies can follow. 1) Does your device improve patient care outcomes? 2) Will it help standardize products, clinical workflow, and care protocols? 3) Will it reduce the contracted price of supplies?
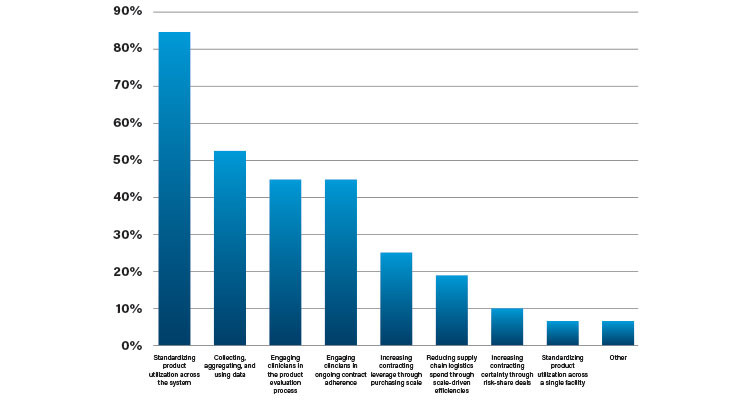
In 2019, Advisory Board conducted a survey that revealed most VACs have three main priorities: expanding oversight over health system-wide purchasing to reduce spend, enhancing data collection abilities, and engaging clinicians throughout and after the value analysis process to ensure clinician satisfaction (Table 1).1
In addition, there were few differences between for-profit vs. non-profit hospitals. Greater differences were seen when comparing different sizes of healthcare organizations; as hospital or IDN size grows, fewer on the VAC in this survey chose price reduction as a top goal for value analysis.
VACs are typically composed of multidisciplinary groups, with each member selected to bring their unique perspective and expertise to the forum. The most frequent participants are operating room managers, supply chain representatives, clinical leaders, and service line leaders.
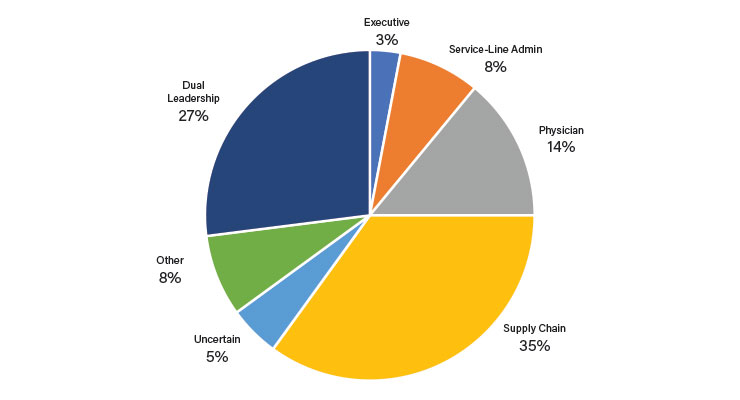
As reflected in Table 2, supply chain representatives are most frequently the leaders of VACs, followed by physicians. A high percentage of physician leadership is seen in VACs that want a clinically integrated supply chain where clinicians have significant input in purchasing decisions.1
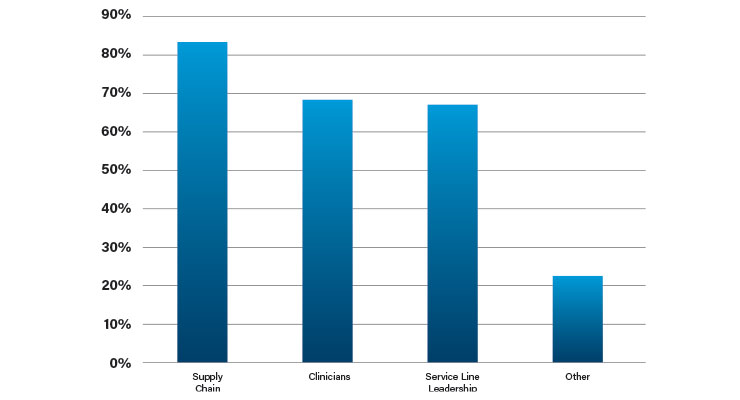
While supply chain representation is the most common leadership model, Table 3 illustrates they don’t wield exclusive decision-making power. As expected, a truly democratic system shows clinicians, supply chain, and service line leaders all have a vote in device and supplier selection.1
Individual VACs tend to be large groups. It is not uncommon for 12 to 24 individuals to sit on a single committee. The roles they represent vary considerably depending on the hospital, the service line, and oftentimes, the specific product under evaluation. Titles include materials manager/purchasing, value assessment analyst, department chairs, nursing, finance, administration, clinical procurement coordinator, and value analysis coordinator.
In terms of internal structure, price sensitivity is affected by the stakeholder chairing the VAC. At organizations where supply chain, purchasing, or finance habitually play this role, it is also more common price discounts will be a chief goal. In organizations where VAC chair duties are aligned to more clinically focused leaders such as physicians, nurses, or service line managers, there is a higher probability clinical outcomes will play a more important role.
Most healthcare organizations have more than one VAC, each specializing in specific types of devices or services.3 In addition, many healthcare organizations assign a VAC to products used within a service line, and if the specific dollar amount warrants it, by product category. One trend slowed but not stopped by the pandemic was the comprehensive, system-wide VAC. This trend is partially due to an increasing pressure to capitalize on operational advantages that come with the formation of larger health systems.
References
Maria Shepherd has more than 20 years of leadership experience in marketing in small startups and top-tier companies. After her industry career, she founded Medi-Vantage, which provides marketing and business strategy and innovation research for the medical device industry. Shepherd can be reached at mshepherd@medi-vantage.com. Visit her website at www.medi-vantage.com.
Why This Is Important
To be successful, hospitals have adopted programs using a multi-disciplinary, data-driven approach to evaluate and source medical devices, capital equipment, disposables, and services. Once a part of the realm of the clinician—usually the doctor, surgeon, or interventionalist—decision-making on devices or capex has shifted to the VAC, which has upended the way suppliers and the medical device industry interact with the broader system of decision makers in the healthcare organization.It's not all about reducing the price of devices. Salespeople need to be versatile in presenting the value of their products and services to the economic or clinical buyer who will likely have many nuanced questions relevant to their functional perspective. Needless to say, it's not as easy as it used to be. However, there are still three main guidelines medical device companies can follow. 1) Does your device improve patient care outcomes? 2) Will it help standardize products, clinical workflow, and care protocols? 3) Will it reduce the contracted price of supplies?
In 2019, Advisory Board conducted a survey that revealed most VACs have three main priorities: expanding oversight over health system-wide purchasing to reduce spend, enhancing data collection abilities, and engaging clinicians throughout and after the value analysis process to ensure clinician satisfaction (Table 1).1
If Not Price Decreases, Then What?
If not price reductions, is improving patient outcomes the driver for VACs? In another pre-COVID-19 survey (n=121), 55% of respondents were segmented as value-focused (reducing price was not in their top three goals) vs. 45% segmented as price-focused (reducing price was a priority and in their top three goals). Significant differences could be observed in the prevalence of other goals that aligned with the value-focused segment. Both segments gave high scores to improving patient outcomes. Differences were seen in lower scores at price-focused VACs for improving patient satisfaction, improving process efficiencies, and advancing staff safety.2In addition, there were few differences between for-profit vs. non-profit hospitals. Greater differences were seen when comparing different sizes of healthcare organizations; as hospital or IDN size grows, fewer on the VAC in this survey chose price reduction as a top goal for value analysis.
VACs are typically composed of multidisciplinary groups, with each member selected to bring their unique perspective and expertise to the forum. The most frequent participants are operating room managers, supply chain representatives, clinical leaders, and service line leaders.
As reflected in Table 2, supply chain representatives are most frequently the leaders of VACs, followed by physicians. A high percentage of physician leadership is seen in VACs that want a clinically integrated supply chain where clinicians have significant input in purchasing decisions.1
While supply chain representation is the most common leadership model, Table 3 illustrates they don’t wield exclusive decision-making power. As expected, a truly democratic system shows clinicians, supply chain, and service line leaders all have a vote in device and supplier selection.1
Individual VACs tend to be large groups. It is not uncommon for 12 to 24 individuals to sit on a single committee. The roles they represent vary considerably depending on the hospital, the service line, and oftentimes, the specific product under evaluation. Titles include materials manager/purchasing, value assessment analyst, department chairs, nursing, finance, administration, clinical procurement coordinator, and value analysis coordinator.
In terms of internal structure, price sensitivity is affected by the stakeholder chairing the VAC. At organizations where supply chain, purchasing, or finance habitually play this role, it is also more common price discounts will be a chief goal. In organizations where VAC chair duties are aligned to more clinically focused leaders such as physicians, nurses, or service line managers, there is a higher probability clinical outcomes will play a more important role.
How Do Vacs Keep Score?
Most hospitals have not coalesced around a single methodology for rating and comparing competing products. The Advisory Board survey found hospitals develop a one-off scorecard for each analysis.1 This is caused by the range of products and services a single committee must evaluate, and the complexity of the devices.Most healthcare organizations have more than one VAC, each specializing in specific types of devices or services.3 In addition, many healthcare organizations assign a VAC to products used within a service line, and if the specific dollar amount warrants it, by product category. One trend slowed but not stopped by the pandemic was the comprehensive, system-wide VAC. This trend is partially due to an increasing pressure to capitalize on operational advantages that come with the formation of larger health systems.
The Medi-Vantage Perspective
These surveys were all performed pre-COVID-19 and Medi-Vantage hospital administrator surveys performed during the pandemic show a shift in thinking by the VAC. In response, our clients have changed the way they perceive the VAC, and the strategies and tools they use to present for their devices, capital equipment, and disposables. Be sure to transform everything your team offers to the clinician into a combined clinical and financial impact, if possible. Avoid competing only on price, which sends the message your product cannot make an adequate clinical case and falls into the death valley of “clinically acceptable,” where the only basis for choosing is price. You have the opportunity to educate your customers and differentiate your devices from competitors by getting ahead of this curve.References
- bit.ly/mpo230301
- bit.ly/mpo230302
- Medi-Vantage internal research
Maria Shepherd has more than 20 years of leadership experience in marketing in small startups and top-tier companies. After her industry career, she founded Medi-Vantage, which provides marketing and business strategy and innovation research for the medical device industry. Shepherd can be reached at mshepherd@medi-vantage.com. Visit her website at www.medi-vantage.com.
