Japan’s Political Shakeup: A New Cabinet Brings New Policy
Yoshio Mitsumori
On Sept. 26, Prime Minister Junichiro Koizume stepped down after five years of service. Succeeding him is Shinzo Abe, who, at 52 years of age, is the youngest prime minister Japan has ever had.
Abe, who had been a chief cabinet secretariat under Koizumi and a supporter of Koizumi’s policies, was first elected as a president of the Liberal Democratic Party (LDP) at its general assembly and then appointed as prime minister at the general Diet session. (The Diet is Japan’s legislature.) After his inauguration, Abe formed his new cabinet on the same day.
Along with Abe’s appointment, 71-year-old Hakuo Yanagisawa, another experienced LDP Diet member, was named the new minister for Health, Labor and Welfare. Yanagisawa, who is widely regarded as a financial expert, previously had served as a minister for Financial Service. Although he has not demonstrated any visible presence in the healthcare arena, Yanagisawa’s newest appointment clearly shows that Prime Minister Abe intends to control social security expenditures—which means pensions and health insurance are sure to be affected.
In particular, the pension issue currently has been a top concern among Japanese people, as they have been demanding a drastic reconstruction of the social security system and reorganization of the Social Insurance Agency. Based on what’s developed with the newest appointments, it appears Prime Minister Abe expects Yanagisawa’s political skill will be a valuable asset in navigating through this very difficult—but important—political issue.
Reimbursement Issues
Could Arise
The catchphrase of Abe’s administration is, “Without change, no growth, no financial improvement,” and the intent behind the catchphrase is to balance the country’s finances by the 2011 fiscal year. To achieve this goal, more than 70% of Japan’s budgetary shortage must be covered by expenditure cuts. Ever-growing pension and healthcare insurance costs—largely a result of the growing elderly population—are, perhaps, the most important issues Abe’s administration will have to handle. Accordingly, many people are concerned that healthcare insurance may be affected.
Behind the scenes of the regime change from Koizumi to Abe, the drastic changes seen for drug pricing under the health insurance program have been under investigation (pharmaceutical products account for about 20% of total medical expenditure). Although drug prices were just revised in April 2006, the government and LDP have begun to investigate the possibility of making additional cuts next April to the reimbursement price for drugs. The re-pricing of the drugs usually occurs once every two years. So, theoretically, the next re-pricing should be in 2008. However, this administration is trying to make it an annual revision. The possible reduction range is a maximum of 10%, with the goal of saving one billion Yen. The pharmaceutical industry and hospital industry strongly oppose this annual re-pricing, and for good reason. In the last decade, 4% to 10% had been cut after every review.
Why should the medical device community care about what’s happening to the pharmaceutical industry? After all, the device sector currently is not being affected by these attempts to cut costs. However, the proposed move to re-price drugs annually must be watched carefully by medical device manufacturers, because they, too, could similarly be affected sooner rather than later.
Healthcare Expenditure Worries
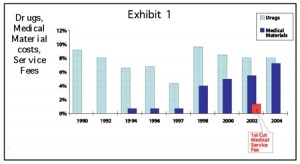
In a more general topic, the Ministry of Health, Labor and Welfare recently made public the general statistics of fiscal 2004’s national healthcare expenditure, which was 32.1 trillion Yen—an increase of 574 billion (1.8%) from 2003. The GDP rate was 8.89%, slightly increased from 8.8% previously (see Figure 1). The expenditure for patients older than 65 years increased 3.3% to 16.4 trillion Yen, which was 51.1% of total expenditures (in 2003, it was 50.4%).
These statistics clearly demonstrate that the increasing elderly population is correlating with the increased healthcare expenditures. For comparison’s sake, the average healthcare expenditure per person only increased 1.8% to 251,500 Yen from 247,100 Yen in 2003. Individuals younger than 65 years spent 152,700 Yen, whereas individuals older than 65 years spent 659,600 Yen.
Looking at healthcare expenditure by service, general hospital/clinic service was 24.3 trillion Yen (75.9% of the total). Within these institutions, in-patient service was 11.8 trillion Yen (36.9%) and outpatient service was 12.5 trillion Yen (39.0%).
Mixed Billing Update:
The Effect on Devices
As we near the end of the year, one more issue of interest deserves examination. It has been more than one year since so-called “Mixed Billing”—the combined medical service for insured and non-insured—was partially permitted in July 2005. The target set was 100 procedures by 2,000 institutions; in reality, after one year of Mixed Billing being instituted, only seven procedures by 63 institutions have been done.
Before Mixed Billing was instituted, if a non-insured medical service would be performed, all medical service fees—even insured services such as accommodations, nursing services and so on—could not be covered by the National Health Insurance, and the patient would have had to pay 100% out of his or her pocket. Mixed Billing, therefore, was expected to reduce the patient’s private burden as well as promote the development of new technology.
Unfortunately, these new technologies haven’t surfaced in spite of the advent of Mixed Billing. Although the application criteria and process have been simplified, new devices and equipment still need to go through the regulatory approval process in advance of being eligible for Mixed Billing.
For example, consider the case of mammoplasty with the use of silicon prosthesis. At present, Japan has had no approved silicon prosthesis. After mastectomy, if a mammoplasty with use of silicon prosthesis is performed, all medical and surgical fees will not be covered by the insurance—and the patient must pay all of them. This market has big demands in Japan, as this prosthesis is a physical and emotional relief for many women who have lost a breast by surgery after breast cancer. However, no supplier promotes this type of prosthesis because the supplier would have to obtain a regulatory approval before marketing it and may need a sizable clinical trial with a big investment involving a four- to five-year timeframe.
In other countries, breast implants are commonly used. In Japan, the only way to conduct the procedure is through the physician’s private import under his or her responsibility. This isn’t easily accomplished, either, when you consider that quantities are limited and, thus, the cost is much more expensive than it might be elsewhere.
The biggest barriers to Mixed Billing working at its full potential is the regulatory approval process and its associated huge investment required for clinical trials. Even though the product cited in our example above has been used extensively globally, Japan needs its own, separate regulatory approval and, often, sizable clinical trials. Many suppliers are rather reluctant to perform these clinical trials as they weigh the return on their investment.
Of course, securing patient safety is a very important administrative measure from the viewpoint of national healthcare management. However, some alternative method is expected for the future. Otherwise, the use of Mixed Billing to reduce a patient’s burden may become only an empty dream.
Yoshio Mitsumori is the president and CEO for Tokyo-based ADMIS, a consultant specializing in the medical device industry. He has more than 25 years of experience in the medical industry, including positions with the Itochu Corp., U.S. Surgical, National Medical Enterprises and Century Medical. A member of RAPS, he has spoken at many industry events and worked extensively in international trade of medical products and technologies. He can be reached at ymitsumori@admis.co.jp.