
Maria Shepherd, President and Founder, Medi-Vantage05.03.21
Many insurance companies don’t cover In Vitro Fertilization (IVF). The financial burdens can be immense. In addition, the complexity of coverage, its cost, and what patients need to receive in time for treatment can be overwhelming. Barbara Collura, president and CEO of Resolve: The National Infertility Association, noted the exclusions on most health plan documents are “typically over 100 pages in teeny tiny font.”1
According to the National Conference of State Legislatures, the average IVF cycle costs between $12,000 and $17,000 (not including medication). The cost of medication can increase the cost of a cycle to $25,000 (Table 1).1 Most clinics define a fertility cycle as one egg retrieval and the embryo transfers that are produced from that retrieval.
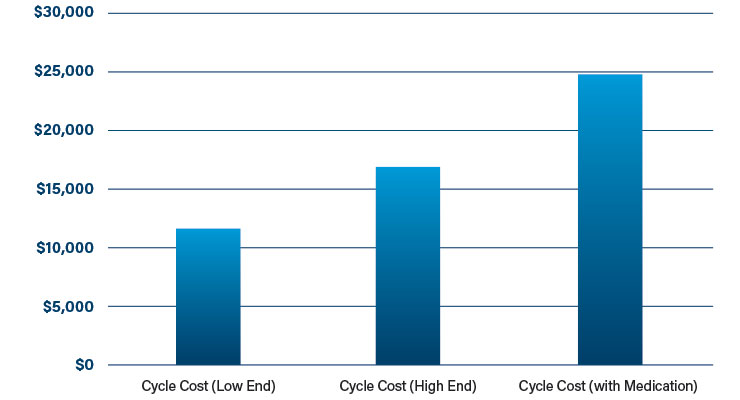
Table 1: Cost of one cycle of fertility treatment1
There are additional costs, such as embryo genetic testing and medical procedures (e.g., sperm extraction, laparoscopy, etc.), which can add thousands of dollars to the cost.
The majority of couples will need more than one series of treatment. The question is how many cycles each couple will need, and the answer is difficult to predict. There have been several clinical studies to determine the answer to this question.
In an Israeli study designed to assess whether the results and effectiveness of unlimited access with IVF in Israel validates the policy of unrestricted IVF (n=535), the rate of success was 54 percent. The study found the success rate declined as the number of unsuccessful cycles and duration of infertility grew. It also determined the age of the mother at the beginning of the treatment was significant.2
In a British study designed to identify the number of infants born per initiated ovarian stimulation IVF cycle and with recurrent cycles (n=156,947), U.K. women who received 257,398 IVF ovarian stimulation cycles were followed.
Among the women in this study, the median age at start of treatment was 35, and the median duration of infertility for all 257,398 cycles was four years. In all the women studied, the live-birth rate for the first cycle was 29.5 percent (Table 2). The live-birth rate remained above 20 percent until the completion of the fourth cycle. The live-birth rate continued to rise to the ninth cycle, with 65.3 percent women achieving a live birth by the sixth cycle. In women less than 40 years old, using their own eggs, the live-birth rate for the first cycle was 32.3 percent and remained above 20 percent up to and including the fourth cycle. Six cycles achieved a live-birth rate of 68.4 percent. For women between 40 and 42 years old, the live-birth rate for the first cycle was 12.3 percent, with six cycles achieving a live-birth rate of 31.5 percent. For women greater than 42 years old, all rates for each cycle were less than four percent.3 This study supported the efficacy of prolonging the number of IVF cycles past three or four.

Table 2: Live births in the first cycle of infertility treatment3
In the U.S., not all fertility treatments are covered, so extending beyond one cycle isn’t financially possible for all couples, explained Lucie Schmidt, Ph.D., a professor of economics at Williams College in Massachusetts. “Some people can afford one cycle on their own, but not two or three.” Dr. Schmidt studies how state insurance directives impact IVF treatment. “Lack of insurance (or less generous insurance) puts additional pressure on women to transfer multiple embryos, which can then lead to costly and risky multiple births.”1
While most multiple births are successful, there can be discomforts and risks. Twins are the most common multiples, and most twin pregnancies are successful. However, pregnancies with twins are frequently more uncomfortable than one-baby pregnancies. A higher level of progesterone means the mother may be short of breath from the beginning of pregnancy. First trimester fatigue can also be significant. As the pregnancy progresses, heartburn and back pain are reported to be worse. Pregnant moms report a higher likelihood of constipation.4
With identical twins, the risk of rare complications can increase. Approximately 10 to 15 percent of identical twins that share a placenta (also called monochorionic twins) can develop a disorder called twin-to-twin transfusion syndrome. When this happens, blood vessels inside the shared placenta send more blood to one twin than to the second. Approximately 70 percent of identical twins are monochorionic, which means the mother will require an ultrasound every two weeks to check on the health of both babies. Treatment choices include early delivery or laser surgery to seal some of the placental blood vessels.4
If the identical twins are monoamniotic, sharing an amniotic sac as well as the placenta (occurs in approximately one percent of identical twins), the umbilical cords of each baby can become twisted, which can flatten them and inhibit blood supply to one or both twins. This risk is also monitored with ultrasound.4
In a study in the American Journal of Obstetrics and Gynecology, 66 percent of pregnancies with twins in the U.S. resulted in a delivery via cesarean section.5 Whether for vaginal or cesarean delivery of multiple babies, most are delivered in the OR. Multiple specialists may be called in—an infant special care team, a pediatrician and nurse for each twin, two midwives, and/or two obstetricians.
And healthcare inequity has an impact. In the journal Fertility and Sterility, it was reported that it may take African-American women a year longer than other ethnicities to seek infertility treatment, and that treatment may be 14 percent less successful than for white patients.6
For those unlucky patients who require the services of an infertility specialist, the number of treatments beyond routine cycle treatments can get very expensive (Table 3). There are multiple technologies for patients that need additional fertility treatments, such as comprehensive chromosome screening, DNA fragmentation index measurement , imaging to assess egg quality, endometrial receptivity arrays, and donor egg banks. Comprehensive chromosome screening is estimated to cost $5,400, while a single donor egg can cost $20,000 and a donor egg guarantee can cost $45,000.7
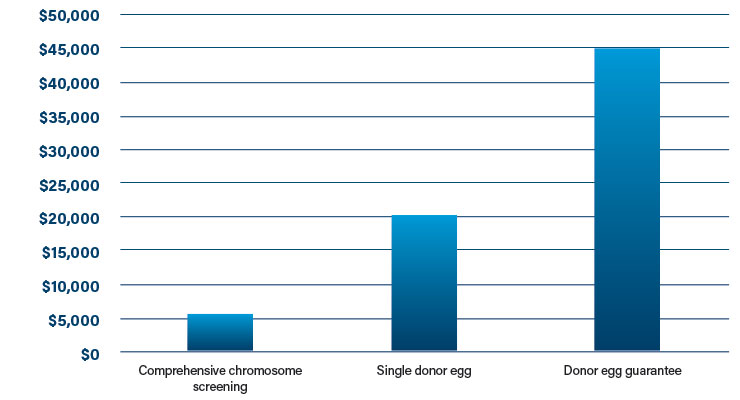
Table 3: Costs of additional treatments to augment IVF7
The Medi-Vantage Perspective
The success rates of fertility treatment have increased over the years, but for those patients 42 years and older, many of the treatments available to expand the success rates of IVF are expensive and not all have been clinically studied, even though they are approved. What is needed here is more patient research to understand the financial impact of infertility treatment, and to offer viable financial options for older prospective parents or those who are fertility impaired who want to have a child.
References
Maria Shepherd has more than 20 years of leadership experience in medical device/life-science marketing in small startups and top-tier companies. After her industry career, she founded Medi-Vantage. Medi-Vantage provides marketing and business strategy and innovation research for the medical device industry. The firm quantitatively and qualitatively sizes and segments opportunities, evaluates new technologies, and assesses prospective acquisitions. Visit her website at www.medi-vantage.com.
According to the National Conference of State Legislatures, the average IVF cycle costs between $12,000 and $17,000 (not including medication). The cost of medication can increase the cost of a cycle to $25,000 (Table 1).1 Most clinics define a fertility cycle as one egg retrieval and the embryo transfers that are produced from that retrieval.
Table 1: Cost of one cycle of fertility treatment1
There are additional costs, such as embryo genetic testing and medical procedures (e.g., sperm extraction, laparoscopy, etc.), which can add thousands of dollars to the cost.
The majority of couples will need more than one series of treatment. The question is how many cycles each couple will need, and the answer is difficult to predict. There have been several clinical studies to determine the answer to this question.
In an Israeli study designed to assess whether the results and effectiveness of unlimited access with IVF in Israel validates the policy of unrestricted IVF (n=535), the rate of success was 54 percent. The study found the success rate declined as the number of unsuccessful cycles and duration of infertility grew. It also determined the age of the mother at the beginning of the treatment was significant.2
In a British study designed to identify the number of infants born per initiated ovarian stimulation IVF cycle and with recurrent cycles (n=156,947), U.K. women who received 257,398 IVF ovarian stimulation cycles were followed.
Among the women in this study, the median age at start of treatment was 35, and the median duration of infertility for all 257,398 cycles was four years. In all the women studied, the live-birth rate for the first cycle was 29.5 percent (Table 2). The live-birth rate remained above 20 percent until the completion of the fourth cycle. The live-birth rate continued to rise to the ninth cycle, with 65.3 percent women achieving a live birth by the sixth cycle. In women less than 40 years old, using their own eggs, the live-birth rate for the first cycle was 32.3 percent and remained above 20 percent up to and including the fourth cycle. Six cycles achieved a live-birth rate of 68.4 percent. For women between 40 and 42 years old, the live-birth rate for the first cycle was 12.3 percent, with six cycles achieving a live-birth rate of 31.5 percent. For women greater than 42 years old, all rates for each cycle were less than four percent.3 This study supported the efficacy of prolonging the number of IVF cycles past three or four.
Table 2: Live births in the first cycle of infertility treatment3
In the U.S., not all fertility treatments are covered, so extending beyond one cycle isn’t financially possible for all couples, explained Lucie Schmidt, Ph.D., a professor of economics at Williams College in Massachusetts. “Some people can afford one cycle on their own, but not two or three.” Dr. Schmidt studies how state insurance directives impact IVF treatment. “Lack of insurance (or less generous insurance) puts additional pressure on women to transfer multiple embryos, which can then lead to costly and risky multiple births.”1
While most multiple births are successful, there can be discomforts and risks. Twins are the most common multiples, and most twin pregnancies are successful. However, pregnancies with twins are frequently more uncomfortable than one-baby pregnancies. A higher level of progesterone means the mother may be short of breath from the beginning of pregnancy. First trimester fatigue can also be significant. As the pregnancy progresses, heartburn and back pain are reported to be worse. Pregnant moms report a higher likelihood of constipation.4
With identical twins, the risk of rare complications can increase. Approximately 10 to 15 percent of identical twins that share a placenta (also called monochorionic twins) can develop a disorder called twin-to-twin transfusion syndrome. When this happens, blood vessels inside the shared placenta send more blood to one twin than to the second. Approximately 70 percent of identical twins are monochorionic, which means the mother will require an ultrasound every two weeks to check on the health of both babies. Treatment choices include early delivery or laser surgery to seal some of the placental blood vessels.4
If the identical twins are monoamniotic, sharing an amniotic sac as well as the placenta (occurs in approximately one percent of identical twins), the umbilical cords of each baby can become twisted, which can flatten them and inhibit blood supply to one or both twins. This risk is also monitored with ultrasound.4
In a study in the American Journal of Obstetrics and Gynecology, 66 percent of pregnancies with twins in the U.S. resulted in a delivery via cesarean section.5 Whether for vaginal or cesarean delivery of multiple babies, most are delivered in the OR. Multiple specialists may be called in—an infant special care team, a pediatrician and nurse for each twin, two midwives, and/or two obstetricians.
And healthcare inequity has an impact. In the journal Fertility and Sterility, it was reported that it may take African-American women a year longer than other ethnicities to seek infertility treatment, and that treatment may be 14 percent less successful than for white patients.6
For those unlucky patients who require the services of an infertility specialist, the number of treatments beyond routine cycle treatments can get very expensive (Table 3). There are multiple technologies for patients that need additional fertility treatments, such as comprehensive chromosome screening, DNA fragmentation index measurement , imaging to assess egg quality, endometrial receptivity arrays, and donor egg banks. Comprehensive chromosome screening is estimated to cost $5,400, while a single donor egg can cost $20,000 and a donor egg guarantee can cost $45,000.7
Table 3: Costs of additional treatments to augment IVF7
The Medi-Vantage Perspective
The success rates of fertility treatment have increased over the years, but for those patients 42 years and older, many of the treatments available to expand the success rates of IVF are expensive and not all have been clinically studied, even though they are approved. What is needed here is more patient research to understand the financial impact of infertility treatment, and to offer viable financial options for older prospective parents or those who are fertility impaired who want to have a child.
References
- bit.ly/mpo210501
- bit.ly/mpo210502
- bit.ly/mpo210503
- bit.ly/mpo210504
- bit.ly/mpo210505
- bit.ly/mpo210506
- Data on file.
Maria Shepherd has more than 20 years of leadership experience in medical device/life-science marketing in small startups and top-tier companies. After her industry career, she founded Medi-Vantage. Medi-Vantage provides marketing and business strategy and innovation research for the medical device industry. The firm quantitatively and qualitatively sizes and segments opportunities, evaluates new technologies, and assesses prospective acquisitions. Visit her website at www.medi-vantage.com.
