

Michael Barbella, Managing Editor04.01.21
Daniel Hawkins caught a glimpse of the future back in 1993.
A newly-minted MBA graduate at the time, Hawkins had recently landed his first job in medtech and was in Chicago for a 48-hour whirlwind round of surgical consults. Both he and a sales rep were scheduled to lend product support in a handful of cases at two different hospitals.
Given his naivety, Hawkins fully expected his jam-packed itinerary to commence as planned.
As if life ever goes according to plan.
Hawkins left the Windy City frustrated, disappointed, and a bit disconcerted. He never made it to the second hospital and only attended to a fraction of the cases.
“I arrived in Chicago, and the mission was to see a case or two that day, have dinner with a doctor, see a whole day of cases the following day, and fly out afterwards,” Hawkins recalled. “It didn’t happen that way. The first case happened the next day, but the next two were canceled and we never made it to the second hospital. As the sales rep was driving me to the airport, she was very apologetic. I was wondering whether this is how it is, so I asked her, ‘Do cases get bumped?’ She said, ‘All the time.’ When I got back, I told my manager how much time we spent running around and how little time we spent in procedure rooms, and he told me that was normal. That really struck me.”
The impression it left forever altered Hawkins’ medtech career. As he advanced in the industry, the logistical issues associated with in-person surgical support became more apparent (and frustrating), yet remained an accepted norm among medical device sales reps. Hawkins claims these folks spend roughly 50-60 percent of their working hours on logistics (travel, procedure prep, and case delays).
Though he tolerated such a nonsensical imbalance, Hawkins never fully accepted it. The frustration he first experienced as a medtech industry rookie only grew with each invention he conceived (more than 140 and counting) and company he joined, finally reaching a boiling point during his tenure leading Shockwave Medical Inc., a firm Hawkins founded in 2012 to develop and commercialize calcified coronary artery disease treatment.
“As a sales rep, you can only see two customers in a day. The logistics will prohibit you from doing any more [cases],” Hawkins noted. “If you make a choice to be at hospital one to support a procedure in the morning, logistically you cannot be at hospital five in the afternoon if that facility is in a location on the other side of your territory. I got frustrated with that as a problem. I saw that problem back in 1993 when I was starting out in the medical device industry and I saw that problem in spades as the founder of Shockwave Medical.”
“When I was with Shockwave Medical I flew multiple times overseas for clinical support cases,” he continued. “As CEO, why did I do that? Well, the physicians needed support and I knew the technology better than anyone. Once, I flew to New Zealand. I landed, went straight to the hospital, left my bags at the nurses’ station, went immediately into the procedure room, did two cases, had dinner with the treating physician, and then flew home. I flew to Austria multiple times and did the same thing but stayed over. It was brutal. Looking at all that, it just doesn’t make any sense. I kept thinking there had to be a better way.”
That better way eventually arose through telemedicine, a relatively newer branch of healthcare that delivers remote patient diagnoses and treatments through telecommunications technology. With roots traceable to the mid-19th century, telemedicine has grown rapidly in the last two decades, having been nourished by the Internet and its cornucopia of digital applications. Those applications (e.g., e-mail, teleconsults, Internet conferences) and multimedia approaches (digital imagery and video) have helped create a rich tapestry of virtual solutions.
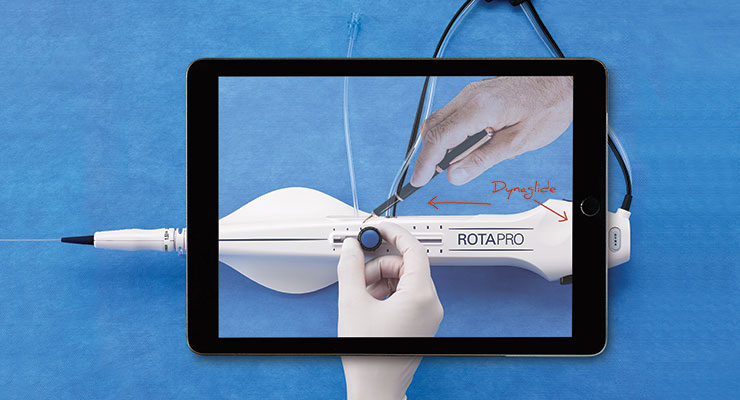
Hawkins’ answer to the logistical headaches in medtech sales, for example, involves remotely connecting reps to the operating room. The company he founded four years ago—Avail Medsystems Inc.—has developed a “procedural telemedicine” system that digitizes physical presence, thereby enabling physicians, healthcare professionals, and sales reps to collaborate virtually during surgical procedures.
The Avail System features a portable console outfitted with high-definition cameras, adjustable arms, and a monitor with a touchscreen interface. Outside experts (including physicians) can virtually consult with the O.R. team during procedures through an app that allows for real-time annotation and other image-control options.
Avail places its consoles in hospitals and ASC facilities for free but charges companies for each minute of use (similar to a cell phone contract). The solution, while not yet widespread, is quickly gaining traction and interest within the healthcare industry: Last fall, the Palo Alto, Calif.-based company raised $100 million in Series B funding and landed a contract with Smith+Nephew plc.
“The notion here is to provide a way for physicians and others to access the O.R. without the logistical burdens and cost burdens of actually being there. This is not a technology designed to replace a [sales] rep,” noted Hawkins, the firm’s CEO. “What it does is makes them more efficient, able to serve more customers, and very importantly, their customers know they have a phone-a-friend option all the time. In many respects we are a consultative facilitation tool. It’s called a practice in medicine for a reason—because nobody achieves perfection. There really should be a fluidity of dialogue, and I’d like Avail to be the connective tissue between all that dialogue. I really see this technology as filling a gap in the telemedicine story.”
The tale, however, currently is undergoing a major revision as the technology assumes a leading role in the overall healthcare narrative. Due in large part to the COVID-19 pandemic, telemedicine has quickly evolved from atypical offering to mainstream treatment model.
Indeed, the coronavirus outbreak proved to be telemedicine’s watershed moment—the mainspring, so to speak, for widespread adoption. Virtual doctor visits rose exponentially at the pandemic’s outset and continued through spring: Various studies found a 20-fold increase in telemedicine use in March 2020 and a 23-fold surge through June 2020. Concurrently, outpatient visits fell 35 percent.
Part of that surge was driven by physicians as they sought ways to treat housebound patients and protect their staff. Industry data shows telemedicine use was most prominent among endocrinologists, gastroenterologists, neurologists, pain management clinicians, psychiatrists, and cardiologists. Specialists who usually require in-person visits also embraced telemedicine services during the height of the pandemic, including orthopedic surgeons, ophthalmologists, physical therapists, and optometrists.
Such extensive adoption of telemedicine last year (physicians and patients alike) helped boost the market’s value a staggering 92 percent to $79.79 billion, according to Fortune Business Insights. The market research and consulting firm predicts the sector to expand 25.8 percent annually through 2027, driven by new government policies, reimbursement guidelines, technological advancements, and continued utilization post-pandemic.
“From an obvious perspective, telemedicine has opened up significant access to care and the ability for patients of all ages to choose from a wide array of clinical services from direct-to-consumer care, scheduled follow-up visits with their own providers as well as acute / hospital care offered by various specialists,” said Dan Olson, senior vice president, Provider and Payer Solutions, for Boston-based telehealth behemoth Amwell. “Our customers turned to many different types of telehealth clinical services and consults during the pandemic. Many realized how telehealth can be an excellent supplement or extension of an in-person visit. I think the journey will continue after the pandemic because of the incredible exposure to telehealth that patients, providers, and other members of the care team have been experiencing.
Telehealth utilization was trending up before last year but the tremendous growth in 2020 exposed so many patients and providers to what is possible. And many appreciated and liked what they experienced.”
Liked it enough, in fact, to continue leveraging the technology post-pandemic. Surveys have shown a keen interest among patients and physicians in maintaining virtual communications going forward. More than three-quarters of healthcare providers, for example, want to continue using telemedicine for chronic disease management, and roughly 70 percent anticipate using virtual platforms for future medical management, a COVID-19 Healthcare Coalition workgroup poll concluded. Moreover, 62 percent of providers are planning to use telemedicine to coordinate care, 55 percent want it for preventative care, and about half fancy it for hospital or emergency room visit follow-ups. Forty-five percent are eyeing up the technology for mental or behavioral health purposes, while 44 percent want it for specialty care.
“The numbers speak for themselves. Telehealth adoption leading up to 2020 had already doubled in the years 2016 to 2019, and that trend is continuing to grow, with industry estimates forecasting increased adoption to between 60 percent and 90 percent,” stated Karsten Russell-Wood, Portfolio Marketing Leader, Home Health, in Philips’ Connected Care business. “It’s clear the ‘digital front door’ is here to stay and virtual first strategies enabled by telehealth, analytics, and communication tools are connecting patients to providers anywhere, anytime. The way patients approach their healthcare is changing, and providers will need to continue offering these technologies to meet them where they are. The technology solutions that will be successful in the future will be those that strengthen the connection between patients and providers, and telehealth can do just that.”
Philips helped reinforce the patient-provider connection last summer by launching its Virtual Care Station, a delivery system for localized telehealth services. The pod-based solution is designed to connect healthcare vendors and insurers in neighborhood settings like libraries, universities, retail shops, and town halls, thus providing patients with increased local care options.
Philips also enhanced the patient-provider relationship last year through collaborations with the American Telemedicine Association and U.S. Department of Veterans Affairs. The company joined forces with the former organization to further grow its own telehealth offerings, and contracted with the latter to expand the agency’s existing telehealth capabilities.
More recently, the company expanded remote patient management capabilities in North America, Europe, and Japan with the release of the Philips Medical Tablet, a portable monitoring kit for remote access to patient data. The tablet uses Philips IntelliVue XDS software to connect wired or wirelessly to hospital systems regardless of whether the device is present.
“With the consumerization of healthcare as well as persistent access to care challenges, care delivery settings are changing. Telehealth provides a shift in care paradigms, bringing expert care to the patient rather than always requiring the patient to travel to visit a clinician,” Russell-Wood noted. “Telehealth has changed the status quo of the traditional PCP-patient relationship, and the entire care continuum needs to shift to meet the modern demands of a healthcare consumer—offering an abundance of choices for how their care is delivered.”
Those care delivery options currently run the gamut from wearable devices and medical apps to virtual consults and remote monitoring technology. Philips has been prolific in the latter category, developing both clinician- and patient-oriented solutions; its eICU program, for example, allows for near real-time remote patient monitoring and early intervention through advanced audio-visual technology. Smart algorithms predict deteriorations in patient health, giving clinicians the ability to remotely communicate with bedside caregivers through live video links, to continuously monitor patient status, and advise on the best treatment course regardless of their physical location.
GE Healthcare offers a similar option to bedside caregivers through its Mural Virtual Care Solution. Besides expanding remote clinical consults and assessments with point-of-care clinicians, Mural gives medical staff remote access to patients’ clinical status and trends, as well as visibility to patient monitoring and ventilation data.
Likewise, Baxter International Inc.’s Sharesource 2.0 clinical portal gives healthcare providers greater insights into patients’ home peritoneal dialysis treatments, and Siemens Healthineers’ myCare Companion software allows healthcare providers to design their own remote care programs for chronic disease patients.
One of Medtronic’s telehealth solutions for monitoring patients at home combines patient engagement technology, care management services, and data analytics and reporting. Patients enrolled in Medtronic Care Management Services (MCMS) monitoring programs for chronic conditions or post-procedure recovery complete routine health checks from home using the InterVIEW mobile platform. They answer condition-specific symptom questions, submit vital signs, and receive education at potential teachable moments. The technology also supports clinician-initiated video visits and in-app messaging. The patient-submitted data is securely transmitted to MCMS’ clinical monitoring software, which alerts the care team if the patient’s data falls outside of established thresholds. This is designed to give insights into patient health over time, allowing providers to identify trends and intervene if needed.
Another example of Medtronic’s telehealth technology can be found in some features of its InterStim system for treating incontinence. Patients with an InterStim system use a device that looks like a common smartphone to remotely manage their therapy. Known as the smart programmer, it is outfitted with Zoom so patients can receive virtual support from their physicians anywhere with Internet connectivity.
“Telemedicine and remote patient monitoring are two telehealth modalities that provide the ‘just-in-time’ vs. ‘just in case’ benefit that supports access, efficiency, and likely effectiveness,” said Sheri Dodd, vice president and general manager of Medtronic Care Management Services. “From a time and efficiency standpoint alone, telemedicine offers ‘on demand’ engagement between patient and clinician, timed to the convenience of the patient. If a patient is under remote monitoring services, the physician and patient engagement is more proactive and timelier, which may result in an avoidance of a hospitalization and more appropriate site of care services. This could save money and is efficient for both the provider and the patient.”
Better efficiency also is practicable through virtual technical support programs. Boston Scientific Corp.’s Ask Angie is a merged reality app that provides integrated training and cath lab clinical support at the push of a button. The app allows users to view clinical applications, setup, and troubleshooting information with on-demand access to a company representative.
The telemedicine portfolio at Boston Scientific includes remote monitoring solutions as well for improved patient outcomes. Its HeartLogic Heart Failure Diagnostic Service provides continuous HF monitoring by combining and evaluating sensor-tracked data of heart sounds, respiration rate and volume, thoracic impedance, heart rate, and activity. A 900-patient study (MultiSENSE) linked the HeartLogic algorithm with a 70 percent sensitivity rate in detecting HF events.
The company’s LATITUDE NXT Remote Patient Management System gives clinicians the ability to monitor their subjects’ device data (transvenous ICDs, CRT-Ds, CRT-Ps, and pacemakers) between scheduled appointments. The solution is compatible with the HeartLogic Diagnostic.
“There are an increasing number of diagnostic tools coming to fruition with telemedicine. There’s everything from blood pressure monitors to pulse oximeters...COVID-19 was an incredible impetus for that—everyone was measuring their pulse oxygen levels to see if they needed to go to the hospital,” stated David Feygin, Ph.D., Boston Scientific’s chief digital officer and IT vice president. “More is being done to augment treatments requiring physical interaction. Hospitals are moving toward providing more services in the home, where patients can check in after surgery or even receive treatment through telehealth. There’s a lot of data that is being generated through telehealth solutions, and it’s all very timely and relevant to the patient. All that data is new, it’s never existed before, and it’s generating some very creative solutions. It’s opening up a world of opportunity.”
That world is not without its challenges, though. One of the major threats to telemedicine’s future growth is the lack of permanent, clearly defined regulations. The U.S. government implemented various temporary policies and relaxed numerous rules to encourage the use of telemedicine during the pandemic (it worked, too—85 percent of medical practices were conducting virtual visits by late April 2020), but many of those interim measures are set to expire when the outbreak ends. Permanent changes will require Congressional legislation in some cases, as well as action by state governments, licensing boards, and private insurers.
Only a handful of states, however, have turned their provisional telehealth rules into permanent policies. Massachusetts was the first, equalizing care standards for both in-person and telemedicine visits last June, and nixing face-to-face pre-requisites for telehealth appointments. Colorado, Idaho, and New Hampshire also have permanentized temporary telemedicine regulations, and the Centers for Medicare & Medicaid Services (CMS) is indefinitely extending coverage to 60 of 144 interim telehealth services, including those for group psychotherapy, cognitive assessment and care planning, psychological and neuropsychological testing, and domiciliary, rest home, or custodial care services for established patients.
In addition, the agency finalized a list of services reimbursable through Dec. 21, 2021, or the end of the calendar year in which the COVID-19 pandemic is over. The services include home visits to established patients; certain emergency room visits; nursing facilities discharge day management; critical care services; inpatient neonatal and pediatric critical care; and physical and occupational therapy services. Moreover, CMS is allowing telehealth visits with interactive audio and video supervision to be covered through December 2021 or the end of the year the pandemic ends.
“There will need to be a careful review of the policies created during the pandemic that allowed for telehealth utilization at scale, followed by determination of which to keep, which to modify, and which to discontinue,” Dodd noted. “Regarding Medicare, we also know that Congress will have to act in order for access to telehealth in patients’ homes, and beyond just rural areas, to continue. CMS is limited in terms of being able to apply many of the waivers that have been so important during the crisis on a permanent basis, even if they wanted to, because of how the federal law is written. Regulation changes from CMS, FCC, and FDA will all be required to maintain the telehealth momentum, and how these policies are shaped will influence the technology that gets developed. Key areas of focus for regulation changes, to name a few, include: data security and privacy; keeping current and having clear delineation between over-the-counter wellness vs. FDA-approved clinical produce use indications; evidence requirements for telehealth solutions that are reimbursed; scope of clinical license to use telehealth solutions and be paid for it; [and] site of care, including the location of the patient in relation to the provider.”
Location is actually another key challenge potentially imperiling telemedicine’s post-pandemic future. Virtual office visits require reliable internet connections with high-speed transmissions, but access to such networks is currently dependent upon geography, income, age, sex, race, and education levels. Studies have shown that older adults, the poor, communities of color, and rural residents are less likely to have access to the necessary technology to conduct a virtual doctor’s visit.
At least 21 million U.S. residents (likely more) lack fixed broadband internet access, relying instead on their mobile devices for connectivity, Harvard Medical School data indicate. Other statistics show that Americans living in urban areas have better access to high-speed fixed service than their counterparts in rural and tribal lands, and more Caucasians are home broadband users compared with Blacks and Hispanics (79 percent vs. 66 percent and 61 percent, respectively, per Pew Research Center figures).
Similar disparities exist in hospitals, too, affecting physicians’ ability to share data between themselves and their patients. Improved interoperability between different electronic systems across the healthcare delivery system is needed to help improve virtual visits and maintain telemedicine’s future growth.
“Telehealth has seen robust growth during the COVID-19 pandemic. To maintain that growth, though, there are specific improvements to telehealth services that we see as key to encouraging everyone in the healthcare ecosystem including patients, physicians, and payers, to continue using and adopting this technology,” said Paul Chaffin, president of Phillips-Medisize, a Molex company, supplier of connectors and interconnect components. “For example, we see a growing need to establish remote monitoring of patient vitals and monitor patient medication adherence as key areas of improvement that physicians are seeking. It will also be increasingly important to link multiple digital data sources to enable a complete picture for providers.”
Data coming from patients’ homes is expected to become more vital as smart devices continue to proliferate the market. Electronics manufacturing services firm Flex launched a software platform three years ago to help healthcare providers better harvest and manage data from connected medical devices and drug delivery systems.
The firm’s BrightInsight platform integrates with electronic health records and other IT systems while driving high-level analytics with dashboards monitoring clinical data, patient, engagement, and more.
“BrightInsight is a good example of the ‘back end’ infrastructure on a SAAS model that streamlines workflow and makes it easy for patients to engage,” John Carlson, president of Flex’s Health Solutions business unit, stated. “The expansion of smart devices will further [telehealth’s] growth and help healthcare move from the hospital to the home. When data can be collected at home and integrated into the care equation, more remote-based care is possible. In addition, common platforms and infrastructure will help physicians to manage workflow, and manage their patients’ drug treatment regimens through telehealth.”
Clearly, the increase in data generated by telemedicine technology will necessitate strong cybersecurity and patient privacy protection measures. Solutions might involve proactively monitoring and auditing unusual billing behaviors related to telehealth services.
Along with stringent cybersecurity measures, telemedicine solutions must incorporate ease-of-use, rapid learning, and past iterations into their designs. Perhaps most importantly for maintaining growth, however, is the ability for these solutions to address current market needs.
“This is true with any technology. You cannot apply the same hammer to everything. You have to apply the right technology to solve specific problems,” explained Sandra Nagale, director of Boston Scientific’s Digital Health Platforms & Products. “The most important thing will be not to slow down right now because there will be many opportunities to find new ways to improve clinical workflows. We’re changing how we work in every space around digital health and with that said, we have to be sure that our technology is addressing the problems at hand. It’s going to be exciting to see how this space evolves further. As hard as this last year has been, we’ve built multiple solutions we can be proud of. If I take a look at where we are now, I can only imagine where we are headed.”
A newly-minted MBA graduate at the time, Hawkins had recently landed his first job in medtech and was in Chicago for a 48-hour whirlwind round of surgical consults. Both he and a sales rep were scheduled to lend product support in a handful of cases at two different hospitals.
Given his naivety, Hawkins fully expected his jam-packed itinerary to commence as planned.
As if life ever goes according to plan.
Hawkins left the Windy City frustrated, disappointed, and a bit disconcerted. He never made it to the second hospital and only attended to a fraction of the cases.
“I arrived in Chicago, and the mission was to see a case or two that day, have dinner with a doctor, see a whole day of cases the following day, and fly out afterwards,” Hawkins recalled. “It didn’t happen that way. The first case happened the next day, but the next two were canceled and we never made it to the second hospital. As the sales rep was driving me to the airport, she was very apologetic. I was wondering whether this is how it is, so I asked her, ‘Do cases get bumped?’ She said, ‘All the time.’ When I got back, I told my manager how much time we spent running around and how little time we spent in procedure rooms, and he told me that was normal. That really struck me.”
The impression it left forever altered Hawkins’ medtech career. As he advanced in the industry, the logistical issues associated with in-person surgical support became more apparent (and frustrating), yet remained an accepted norm among medical device sales reps. Hawkins claims these folks spend roughly 50-60 percent of their working hours on logistics (travel, procedure prep, and case delays).
Though he tolerated such a nonsensical imbalance, Hawkins never fully accepted it. The frustration he first experienced as a medtech industry rookie only grew with each invention he conceived (more than 140 and counting) and company he joined, finally reaching a boiling point during his tenure leading Shockwave Medical Inc., a firm Hawkins founded in 2012 to develop and commercialize calcified coronary artery disease treatment.
“As a sales rep, you can only see two customers in a day. The logistics will prohibit you from doing any more [cases],” Hawkins noted. “If you make a choice to be at hospital one to support a procedure in the morning, logistically you cannot be at hospital five in the afternoon if that facility is in a location on the other side of your territory. I got frustrated with that as a problem. I saw that problem back in 1993 when I was starting out in the medical device industry and I saw that problem in spades as the founder of Shockwave Medical.”
“When I was with Shockwave Medical I flew multiple times overseas for clinical support cases,” he continued. “As CEO, why did I do that? Well, the physicians needed support and I knew the technology better than anyone. Once, I flew to New Zealand. I landed, went straight to the hospital, left my bags at the nurses’ station, went immediately into the procedure room, did two cases, had dinner with the treating physician, and then flew home. I flew to Austria multiple times and did the same thing but stayed over. It was brutal. Looking at all that, it just doesn’t make any sense. I kept thinking there had to be a better way.”
That better way eventually arose through telemedicine, a relatively newer branch of healthcare that delivers remote patient diagnoses and treatments through telecommunications technology. With roots traceable to the mid-19th century, telemedicine has grown rapidly in the last two decades, having been nourished by the Internet and its cornucopia of digital applications. Those applications (e.g., e-mail, teleconsults, Internet conferences) and multimedia approaches (digital imagery and video) have helped create a rich tapestry of virtual solutions.
Hawkins’ answer to the logistical headaches in medtech sales, for example, involves remotely connecting reps to the operating room. The company he founded four years ago—Avail Medsystems Inc.—has developed a “procedural telemedicine” system that digitizes physical presence, thereby enabling physicians, healthcare professionals, and sales reps to collaborate virtually during surgical procedures.
The Avail System features a portable console outfitted with high-definition cameras, adjustable arms, and a monitor with a touchscreen interface. Outside experts (including physicians) can virtually consult with the O.R. team during procedures through an app that allows for real-time annotation and other image-control options.
Avail places its consoles in hospitals and ASC facilities for free but charges companies for each minute of use (similar to a cell phone contract). The solution, while not yet widespread, is quickly gaining traction and interest within the healthcare industry: Last fall, the Palo Alto, Calif.-based company raised $100 million in Series B funding and landed a contract with Smith+Nephew plc.
“The notion here is to provide a way for physicians and others to access the O.R. without the logistical burdens and cost burdens of actually being there. This is not a technology designed to replace a [sales] rep,” noted Hawkins, the firm’s CEO. “What it does is makes them more efficient, able to serve more customers, and very importantly, their customers know they have a phone-a-friend option all the time. In many respects we are a consultative facilitation tool. It’s called a practice in medicine for a reason—because nobody achieves perfection. There really should be a fluidity of dialogue, and I’d like Avail to be the connective tissue between all that dialogue. I really see this technology as filling a gap in the telemedicine story.”
The tale, however, currently is undergoing a major revision as the technology assumes a leading role in the overall healthcare narrative. Due in large part to the COVID-19 pandemic, telemedicine has quickly evolved from atypical offering to mainstream treatment model.
Indeed, the coronavirus outbreak proved to be telemedicine’s watershed moment—the mainspring, so to speak, for widespread adoption. Virtual doctor visits rose exponentially at the pandemic’s outset and continued through spring: Various studies found a 20-fold increase in telemedicine use in March 2020 and a 23-fold surge through June 2020. Concurrently, outpatient visits fell 35 percent.
Part of that surge was driven by physicians as they sought ways to treat housebound patients and protect their staff. Industry data shows telemedicine use was most prominent among endocrinologists, gastroenterologists, neurologists, pain management clinicians, psychiatrists, and cardiologists. Specialists who usually require in-person visits also embraced telemedicine services during the height of the pandemic, including orthopedic surgeons, ophthalmologists, physical therapists, and optometrists.
Such extensive adoption of telemedicine last year (physicians and patients alike) helped boost the market’s value a staggering 92 percent to $79.79 billion, according to Fortune Business Insights. The market research and consulting firm predicts the sector to expand 25.8 percent annually through 2027, driven by new government policies, reimbursement guidelines, technological advancements, and continued utilization post-pandemic.
“From an obvious perspective, telemedicine has opened up significant access to care and the ability for patients of all ages to choose from a wide array of clinical services from direct-to-consumer care, scheduled follow-up visits with their own providers as well as acute / hospital care offered by various specialists,” said Dan Olson, senior vice president, Provider and Payer Solutions, for Boston-based telehealth behemoth Amwell. “Our customers turned to many different types of telehealth clinical services and consults during the pandemic. Many realized how telehealth can be an excellent supplement or extension of an in-person visit. I think the journey will continue after the pandemic because of the incredible exposure to telehealth that patients, providers, and other members of the care team have been experiencing.
Telehealth utilization was trending up before last year but the tremendous growth in 2020 exposed so many patients and providers to what is possible. And many appreciated and liked what they experienced.”
Liked it enough, in fact, to continue leveraging the technology post-pandemic. Surveys have shown a keen interest among patients and physicians in maintaining virtual communications going forward. More than three-quarters of healthcare providers, for example, want to continue using telemedicine for chronic disease management, and roughly 70 percent anticipate using virtual platforms for future medical management, a COVID-19 Healthcare Coalition workgroup poll concluded. Moreover, 62 percent of providers are planning to use telemedicine to coordinate care, 55 percent want it for preventative care, and about half fancy it for hospital or emergency room visit follow-ups. Forty-five percent are eyeing up the technology for mental or behavioral health purposes, while 44 percent want it for specialty care.
“The numbers speak for themselves. Telehealth adoption leading up to 2020 had already doubled in the years 2016 to 2019, and that trend is continuing to grow, with industry estimates forecasting increased adoption to between 60 percent and 90 percent,” stated Karsten Russell-Wood, Portfolio Marketing Leader, Home Health, in Philips’ Connected Care business. “It’s clear the ‘digital front door’ is here to stay and virtual first strategies enabled by telehealth, analytics, and communication tools are connecting patients to providers anywhere, anytime. The way patients approach their healthcare is changing, and providers will need to continue offering these technologies to meet them where they are. The technology solutions that will be successful in the future will be those that strengthen the connection between patients and providers, and telehealth can do just that.”
Philips helped reinforce the patient-provider connection last summer by launching its Virtual Care Station, a delivery system for localized telehealth services. The pod-based solution is designed to connect healthcare vendors and insurers in neighborhood settings like libraries, universities, retail shops, and town halls, thus providing patients with increased local care options.
Philips also enhanced the patient-provider relationship last year through collaborations with the American Telemedicine Association and U.S. Department of Veterans Affairs. The company joined forces with the former organization to further grow its own telehealth offerings, and contracted with the latter to expand the agency’s existing telehealth capabilities.
More recently, the company expanded remote patient management capabilities in North America, Europe, and Japan with the release of the Philips Medical Tablet, a portable monitoring kit for remote access to patient data. The tablet uses Philips IntelliVue XDS software to connect wired or wirelessly to hospital systems regardless of whether the device is present.
“With the consumerization of healthcare as well as persistent access to care challenges, care delivery settings are changing. Telehealth provides a shift in care paradigms, bringing expert care to the patient rather than always requiring the patient to travel to visit a clinician,” Russell-Wood noted. “Telehealth has changed the status quo of the traditional PCP-patient relationship, and the entire care continuum needs to shift to meet the modern demands of a healthcare consumer—offering an abundance of choices for how their care is delivered.”
Those care delivery options currently run the gamut from wearable devices and medical apps to virtual consults and remote monitoring technology. Philips has been prolific in the latter category, developing both clinician- and patient-oriented solutions; its eICU program, for example, allows for near real-time remote patient monitoring and early intervention through advanced audio-visual technology. Smart algorithms predict deteriorations in patient health, giving clinicians the ability to remotely communicate with bedside caregivers through live video links, to continuously monitor patient status, and advise on the best treatment course regardless of their physical location.
GE Healthcare offers a similar option to bedside caregivers through its Mural Virtual Care Solution. Besides expanding remote clinical consults and assessments with point-of-care clinicians, Mural gives medical staff remote access to patients’ clinical status and trends, as well as visibility to patient monitoring and ventilation data.
Likewise, Baxter International Inc.’s Sharesource 2.0 clinical portal gives healthcare providers greater insights into patients’ home peritoneal dialysis treatments, and Siemens Healthineers’ myCare Companion software allows healthcare providers to design their own remote care programs for chronic disease patients.
One of Medtronic’s telehealth solutions for monitoring patients at home combines patient engagement technology, care management services, and data analytics and reporting. Patients enrolled in Medtronic Care Management Services (MCMS) monitoring programs for chronic conditions or post-procedure recovery complete routine health checks from home using the InterVIEW mobile platform. They answer condition-specific symptom questions, submit vital signs, and receive education at potential teachable moments. The technology also supports clinician-initiated video visits and in-app messaging. The patient-submitted data is securely transmitted to MCMS’ clinical monitoring software, which alerts the care team if the patient’s data falls outside of established thresholds. This is designed to give insights into patient health over time, allowing providers to identify trends and intervene if needed.
Another example of Medtronic’s telehealth technology can be found in some features of its InterStim system for treating incontinence. Patients with an InterStim system use a device that looks like a common smartphone to remotely manage their therapy. Known as the smart programmer, it is outfitted with Zoom so patients can receive virtual support from their physicians anywhere with Internet connectivity.
“Telemedicine and remote patient monitoring are two telehealth modalities that provide the ‘just-in-time’ vs. ‘just in case’ benefit that supports access, efficiency, and likely effectiveness,” said Sheri Dodd, vice president and general manager of Medtronic Care Management Services. “From a time and efficiency standpoint alone, telemedicine offers ‘on demand’ engagement between patient and clinician, timed to the convenience of the patient. If a patient is under remote monitoring services, the physician and patient engagement is more proactive and timelier, which may result in an avoidance of a hospitalization and more appropriate site of care services. This could save money and is efficient for both the provider and the patient.”
Better efficiency also is practicable through virtual technical support programs. Boston Scientific Corp.’s Ask Angie is a merged reality app that provides integrated training and cath lab clinical support at the push of a button. The app allows users to view clinical applications, setup, and troubleshooting information with on-demand access to a company representative.
The telemedicine portfolio at Boston Scientific includes remote monitoring solutions as well for improved patient outcomes. Its HeartLogic Heart Failure Diagnostic Service provides continuous HF monitoring by combining and evaluating sensor-tracked data of heart sounds, respiration rate and volume, thoracic impedance, heart rate, and activity. A 900-patient study (MultiSENSE) linked the HeartLogic algorithm with a 70 percent sensitivity rate in detecting HF events.
The company’s LATITUDE NXT Remote Patient Management System gives clinicians the ability to monitor their subjects’ device data (transvenous ICDs, CRT-Ds, CRT-Ps, and pacemakers) between scheduled appointments. The solution is compatible with the HeartLogic Diagnostic.
“There are an increasing number of diagnostic tools coming to fruition with telemedicine. There’s everything from blood pressure monitors to pulse oximeters...COVID-19 was an incredible impetus for that—everyone was measuring their pulse oxygen levels to see if they needed to go to the hospital,” stated David Feygin, Ph.D., Boston Scientific’s chief digital officer and IT vice president. “More is being done to augment treatments requiring physical interaction. Hospitals are moving toward providing more services in the home, where patients can check in after surgery or even receive treatment through telehealth. There’s a lot of data that is being generated through telehealth solutions, and it’s all very timely and relevant to the patient. All that data is new, it’s never existed before, and it’s generating some very creative solutions. It’s opening up a world of opportunity.”
That world is not without its challenges, though. One of the major threats to telemedicine’s future growth is the lack of permanent, clearly defined regulations. The U.S. government implemented various temporary policies and relaxed numerous rules to encourage the use of telemedicine during the pandemic (it worked, too—85 percent of medical practices were conducting virtual visits by late April 2020), but many of those interim measures are set to expire when the outbreak ends. Permanent changes will require Congressional legislation in some cases, as well as action by state governments, licensing boards, and private insurers.
Only a handful of states, however, have turned their provisional telehealth rules into permanent policies. Massachusetts was the first, equalizing care standards for both in-person and telemedicine visits last June, and nixing face-to-face pre-requisites for telehealth appointments. Colorado, Idaho, and New Hampshire also have permanentized temporary telemedicine regulations, and the Centers for Medicare & Medicaid Services (CMS) is indefinitely extending coverage to 60 of 144 interim telehealth services, including those for group psychotherapy, cognitive assessment and care planning, psychological and neuropsychological testing, and domiciliary, rest home, or custodial care services for established patients.
In addition, the agency finalized a list of services reimbursable through Dec. 21, 2021, or the end of the calendar year in which the COVID-19 pandemic is over. The services include home visits to established patients; certain emergency room visits; nursing facilities discharge day management; critical care services; inpatient neonatal and pediatric critical care; and physical and occupational therapy services. Moreover, CMS is allowing telehealth visits with interactive audio and video supervision to be covered through December 2021 or the end of the year the pandemic ends.
“There will need to be a careful review of the policies created during the pandemic that allowed for telehealth utilization at scale, followed by determination of which to keep, which to modify, and which to discontinue,” Dodd noted. “Regarding Medicare, we also know that Congress will have to act in order for access to telehealth in patients’ homes, and beyond just rural areas, to continue. CMS is limited in terms of being able to apply many of the waivers that have been so important during the crisis on a permanent basis, even if they wanted to, because of how the federal law is written. Regulation changes from CMS, FCC, and FDA will all be required to maintain the telehealth momentum, and how these policies are shaped will influence the technology that gets developed. Key areas of focus for regulation changes, to name a few, include: data security and privacy; keeping current and having clear delineation between over-the-counter wellness vs. FDA-approved clinical produce use indications; evidence requirements for telehealth solutions that are reimbursed; scope of clinical license to use telehealth solutions and be paid for it; [and] site of care, including the location of the patient in relation to the provider.”
Location is actually another key challenge potentially imperiling telemedicine’s post-pandemic future. Virtual office visits require reliable internet connections with high-speed transmissions, but access to such networks is currently dependent upon geography, income, age, sex, race, and education levels. Studies have shown that older adults, the poor, communities of color, and rural residents are less likely to have access to the necessary technology to conduct a virtual doctor’s visit.
At least 21 million U.S. residents (likely more) lack fixed broadband internet access, relying instead on their mobile devices for connectivity, Harvard Medical School data indicate. Other statistics show that Americans living in urban areas have better access to high-speed fixed service than their counterparts in rural and tribal lands, and more Caucasians are home broadband users compared with Blacks and Hispanics (79 percent vs. 66 percent and 61 percent, respectively, per Pew Research Center figures).
Similar disparities exist in hospitals, too, affecting physicians’ ability to share data between themselves and their patients. Improved interoperability between different electronic systems across the healthcare delivery system is needed to help improve virtual visits and maintain telemedicine’s future growth.
“Telehealth has seen robust growth during the COVID-19 pandemic. To maintain that growth, though, there are specific improvements to telehealth services that we see as key to encouraging everyone in the healthcare ecosystem including patients, physicians, and payers, to continue using and adopting this technology,” said Paul Chaffin, president of Phillips-Medisize, a Molex company, supplier of connectors and interconnect components. “For example, we see a growing need to establish remote monitoring of patient vitals and monitor patient medication adherence as key areas of improvement that physicians are seeking. It will also be increasingly important to link multiple digital data sources to enable a complete picture for providers.”
Data coming from patients’ homes is expected to become more vital as smart devices continue to proliferate the market. Electronics manufacturing services firm Flex launched a software platform three years ago to help healthcare providers better harvest and manage data from connected medical devices and drug delivery systems.
The firm’s BrightInsight platform integrates with electronic health records and other IT systems while driving high-level analytics with dashboards monitoring clinical data, patient, engagement, and more.
“BrightInsight is a good example of the ‘back end’ infrastructure on a SAAS model that streamlines workflow and makes it easy for patients to engage,” John Carlson, president of Flex’s Health Solutions business unit, stated. “The expansion of smart devices will further [telehealth’s] growth and help healthcare move from the hospital to the home. When data can be collected at home and integrated into the care equation, more remote-based care is possible. In addition, common platforms and infrastructure will help physicians to manage workflow, and manage their patients’ drug treatment regimens through telehealth.”
Clearly, the increase in data generated by telemedicine technology will necessitate strong cybersecurity and patient privacy protection measures. Solutions might involve proactively monitoring and auditing unusual billing behaviors related to telehealth services.
Along with stringent cybersecurity measures, telemedicine solutions must incorporate ease-of-use, rapid learning, and past iterations into their designs. Perhaps most importantly for maintaining growth, however, is the ability for these solutions to address current market needs.
“This is true with any technology. You cannot apply the same hammer to everything. You have to apply the right technology to solve specific problems,” explained Sandra Nagale, director of Boston Scientific’s Digital Health Platforms & Products. “The most important thing will be not to slow down right now because there will be many opportunities to find new ways to improve clinical workflows. We’re changing how we work in every space around digital health and with that said, we have to be sure that our technology is addressing the problems at hand. It’s going to be exciting to see how this space evolves further. As hard as this last year has been, we’ve built multiple solutions we can be proud of. If I take a look at where we are now, I can only imagine where we are headed.”















