Michael Barbella, Managing Editor06.09.16
It almost worked.
UnitedHealthcare nearly succeeded in keeping its latest policy change under wraps until implementation, surreptitiously disclosing the directive on the seventh page of a lengthy document sent to doctors and patients in early May. Were it not for the fastidiousness of a medtech rival (who gladly spread the word), UnitedHealthcare’s diabetic enrollees might never have known the insurer had chosen Medtronic plc as its preferred insulin pump supplier beginning July 1.
Exclusivity agreements, of course, are not uncommon among insurers and healthcare providers. Case in point: AbbVie in late 2014 forged an exclusive pact with Express Scripts for its new hepatitis C treatment, Viekira Pak, offering the pharmacy benefits manager an undisclosed discount off its $84,000 list price. The deal set off a pricing war with Gilead Sciences Inc., which previously had a lock on the market; the biopharmaceutical giant, however, quickly negotiated its own agreements with Anthem and Humana.
A similar face-off occurred last fall as Amgen Inc., Sanofi, and Regeneron Pharmaceuticals Inc. jockeyed for deals in the market share battle among rival PCSK9 cholesterol-lowering inhibitors. Amgen won that skirmish, nailing exclusive agreements with both CVS Health and Harvard Pilgrim HealthCare by pledging to tie its drug price to efficacy.
Each of the victories, naturally, spawned resentment and controversy within the pharmaceutical industry. Some analysts and physicians claimed Express Scripts’ effort to curb escalating drug costs is also limiting patients’ treatment options. “The issue is what kind of precedent this will create,” Robert Klitzman, an ethics expert at the Columbia University Mailman School of Public Health, told The Wall Street Journal last winter. “We’re going down a path where pharmacy managers, not clinicians, make treatment decisions. Ethically, that’s not the way society ought to make those decisions.”
Klitzman’s disapproval is now being echoed in the diabetes community, where opposition is mounting to the UnitedHealthcare (UHC)-Medtronic pact. An online petition, “Get UnitedHealthcare to Cover all Insulin Pumps,” has garnered nearly 5,000 signatures so far, and patients have been expressing their outrage on social media, using hashtags like #DiabetesAccessMatters, #PatientsOverProfits, and #MyPumpChoice. “It wasn’t my CHOICE to be diabetic (T1 since I was 10), but my care should be my choice. Not yours,” Twitter user and Type 1 diabetic Angela Harlowski tweeted on May 5. “Devices aren’t drugs: Insurance companies should not dictate diabetes technology,” Bea Sparks tweeted the same day.
Sparks’ tweet seemed to best capture the sentiment among many diabetics and professional organizations. A May 10 statement posted on the American Diabetes Association website supports patients’ “critical” right to choose their own pumps: “We know that a single therapeutic approach does not and will not work for all people with diabetes. Partnerships between insurers and vendors that limit therapeutic choices may impair a patient’s access to certain treatments and tools, and adversely affect patient outcomes.”
UHC spokeswoman Kristen A. Hellmer contends the new insulin pump policy was driven by patient safety, service, and cost. She cited the 2012 ASPIRE study, which found that pumps with a low-glucose threshold-suspend feature—currently available only from Medtronic—can help reduce the frequency and duration of hypoglycemic events (low blood sugar).
UHC also claims to base its new policy on member choice (the irony is bound to further rile the masses). A digital fact sheet explaining the UHC-Medtronic relationship indicates that most UnitedHealthcare members use Medtronic insulin pumps more than any other brand; less than 2,500 requests are submitted annually for other manufacturers’ devices (excluding children 18 and younger and Medicare plans).
The fact sheet also detailed the insurer’s policy exemptions. Anyone with a non-Medtronic pump still under warranty will have supplies covered as long as the device is working. Children under 18 are exempt from the exclusivity deal, as are those in Medicare Advantage and UHC Sierra Health or Life Commercial plans.
There will also be a clinical exemption process, according to Hellmer. “If a patient and his/her doctor feel there is a medical need to use a non-Medtronic pump, we will work directly with the prescribing physician on the request,” Hellmer said in an email to the American Journal of Managed Care. Approved requests would be covered as an in-network benefit, she noted.
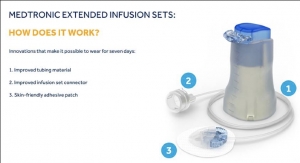
Covered pumps under the new policy include Medtronic’s MiniMed 530G, introduced more than two years ago with great fanfare for its integrated pump and continuous glucose monitoring system with Threshold Suspend, a feature that temporarily shuts off insulin delivery if sensors show glucose levels falling below a preset level.
“Pushing for additional innovation in diabetes care is at the heart of this relationship,” Hellmer told the AJMC. “That is why we plan to bring our experience creating value-based programs with hospitals and physicians to our agreement with Medtronic and hope to expand the industry’s innovation on both technology and clinical programs.”
Diabetes advocates and diabetics, however, fear UHC’s pact with Medtronic will stifle rather than foster innovation in the field. They also say UHC fails to recognize the limiting nature of its new policy.
“Having diabetes isn’t a choice. How people manage it should be,” said Kim Blickenstaff, president and CEO of Tandem Diabetes Care, the company that publicly disclosed the UHC-Medtronic pact. “Insulin pumps are not a one-size fits all solution. Selecting which pump is the best fit for a person to manage their therapy needs should be a decision made between a person and their healthcare provider.”
UnitedHealthcare nearly succeeded in keeping its latest policy change under wraps until implementation, surreptitiously disclosing the directive on the seventh page of a lengthy document sent to doctors and patients in early May. Were it not for the fastidiousness of a medtech rival (who gladly spread the word), UnitedHealthcare’s diabetic enrollees might never have known the insurer had chosen Medtronic plc as its preferred insulin pump supplier beginning July 1.
Exclusivity agreements, of course, are not uncommon among insurers and healthcare providers. Case in point: AbbVie in late 2014 forged an exclusive pact with Express Scripts for its new hepatitis C treatment, Viekira Pak, offering the pharmacy benefits manager an undisclosed discount off its $84,000 list price. The deal set off a pricing war with Gilead Sciences Inc., which previously had a lock on the market; the biopharmaceutical giant, however, quickly negotiated its own agreements with Anthem and Humana.
A similar face-off occurred last fall as Amgen Inc., Sanofi, and Regeneron Pharmaceuticals Inc. jockeyed for deals in the market share battle among rival PCSK9 cholesterol-lowering inhibitors. Amgen won that skirmish, nailing exclusive agreements with both CVS Health and Harvard Pilgrim HealthCare by pledging to tie its drug price to efficacy.
Each of the victories, naturally, spawned resentment and controversy within the pharmaceutical industry. Some analysts and physicians claimed Express Scripts’ effort to curb escalating drug costs is also limiting patients’ treatment options. “The issue is what kind of precedent this will create,” Robert Klitzman, an ethics expert at the Columbia University Mailman School of Public Health, told The Wall Street Journal last winter. “We’re going down a path where pharmacy managers, not clinicians, make treatment decisions. Ethically, that’s not the way society ought to make those decisions.”
Klitzman’s disapproval is now being echoed in the diabetes community, where opposition is mounting to the UnitedHealthcare (UHC)-Medtronic pact. An online petition, “Get UnitedHealthcare to Cover all Insulin Pumps,” has garnered nearly 5,000 signatures so far, and patients have been expressing their outrage on social media, using hashtags like #DiabetesAccessMatters, #PatientsOverProfits, and #MyPumpChoice. “It wasn’t my CHOICE to be diabetic (T1 since I was 10), but my care should be my choice. Not yours,” Twitter user and Type 1 diabetic Angela Harlowski tweeted on May 5. “Devices aren’t drugs: Insurance companies should not dictate diabetes technology,” Bea Sparks tweeted the same day.
Sparks’ tweet seemed to best capture the sentiment among many diabetics and professional organizations. A May 10 statement posted on the American Diabetes Association website supports patients’ “critical” right to choose their own pumps: “We know that a single therapeutic approach does not and will not work for all people with diabetes. Partnerships between insurers and vendors that limit therapeutic choices may impair a patient’s access to certain treatments and tools, and adversely affect patient outcomes.”
UHC spokeswoman Kristen A. Hellmer contends the new insulin pump policy was driven by patient safety, service, and cost. She cited the 2012 ASPIRE study, which found that pumps with a low-glucose threshold-suspend feature—currently available only from Medtronic—can help reduce the frequency and duration of hypoglycemic events (low blood sugar).
UHC also claims to base its new policy on member choice (the irony is bound to further rile the masses). A digital fact sheet explaining the UHC-Medtronic relationship indicates that most UnitedHealthcare members use Medtronic insulin pumps more than any other brand; less than 2,500 requests are submitted annually for other manufacturers’ devices (excluding children 18 and younger and Medicare plans).
The fact sheet also detailed the insurer’s policy exemptions. Anyone with a non-Medtronic pump still under warranty will have supplies covered as long as the device is working. Children under 18 are exempt from the exclusivity deal, as are those in Medicare Advantage and UHC Sierra Health or Life Commercial plans.
There will also be a clinical exemption process, according to Hellmer. “If a patient and his/her doctor feel there is a medical need to use a non-Medtronic pump, we will work directly with the prescribing physician on the request,” Hellmer said in an email to the American Journal of Managed Care. Approved requests would be covered as an in-network benefit, she noted.
Covered pumps under the new policy include Medtronic’s MiniMed 530G, introduced more than two years ago with great fanfare for its integrated pump and continuous glucose monitoring system with Threshold Suspend, a feature that temporarily shuts off insulin delivery if sensors show glucose levels falling below a preset level.
“Pushing for additional innovation in diabetes care is at the heart of this relationship,” Hellmer told the AJMC. “That is why we plan to bring our experience creating value-based programs with hospitals and physicians to our agreement with Medtronic and hope to expand the industry’s innovation on both technology and clinical programs.”
Diabetes advocates and diabetics, however, fear UHC’s pact with Medtronic will stifle rather than foster innovation in the field. They also say UHC fails to recognize the limiting nature of its new policy.
“Having diabetes isn’t a choice. How people manage it should be,” said Kim Blickenstaff, president and CEO of Tandem Diabetes Care, the company that publicly disclosed the UHC-Medtronic pact. “Insulin pumps are not a one-size fits all solution. Selecting which pump is the best fit for a person to manage their therapy needs should be a decision made between a person and their healthcare provider.”