Christopher Delporte, Editorial Director02.14.14
The renal denervation market for high blood pressure: More than a few industry-watchers, medical device companies and analysts have had their eyes on this prize. The potential of a patient population with high blood pressure—clinically called hypertension—that doesn’t respond to traditional pharmaceutical therapies would be enough to make any medical device company take notice. And of course, many did—large firms and start-ups alike.
In fact, many start-ups jumped on the renal denervation bandwagon only to be snatched up (often for hundreds of millions of dollars) by the likes of Medtronic Inc. and Boston Scientific Corp.
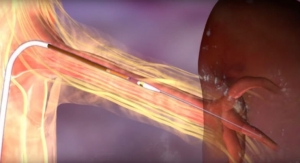
Similar to angioplasty, renal denervation involves snaking a catheter through the femoral artery up to the renal arteries, where it uses heat to deactivate the renal nerves (in the kidneys) which, in theory, lowers blood pressure. Hypertension is associated with an overactive sympathetic drive and renal denervation is the ablation of the renal nerves to stop the “talk” between the kidneys and the brain, thus reducing the sympathetic drive. Congestive heart failure, left ventricular hypertrophy, atrial fibrillation, obstructive sleep apnea, and insulin-resistant type 2 diabetes also are associated with an overactive sympathetic drive. Current clinical trials are researching the effect of renal denervation in these clinical conditions as well, according to RDNworld.com.
The prospects—according to industry number crunchers—for steadily increasing sales in the renal denervation market for hypertension have seemed relatively certain. As recently as December 2013, a report from industry research firm Global Data predicted that the global renal denervation market would grow from $15.5 million in 2012 to $171.7 million by 2019 at a compound annual growth rate of 41 percent, driven by the technology’s approval in major countries, including the United States, by the end of 2019.
What a difference a month can make.
Medtronic Puts on the Brakes
On Jan. 9, Medtronic announced that it would discontinue its third renal denervation study, ending a large U.S. trial for its
Symplicity renal denervation system. The trial, Symplicity HTN-3, met its primary safety endpoint related to the incidence of major adverse events, but it did not meet its primary efficacy endpoint of a change in office blood pressure from baseline to six months. The company claims it was the most rigorous renal denervation study to date.
The Symplicity HTN-1 and HTN-2 trials also demonstrated a good safety profile for catheter-based renal denervation.
While certainly a blow for the Minneapolis, Minn.-based medtech behemoth, the news has a wider industry impact and puts in doubt the future of renal denervation, and what some analysts predicted ultimately could become a billion-dollar worldwide market. According to Medtronic, roughly 1.2 billion people worldwide suffer from high blood pressure and about one-third don’t respond to medication.
In addition to ending the trial, which involved 535 patients at 87 medical centers throughout the United States, Medtronic also stopped recruiting patients for clinical trials in Japan and India. In Europe, the Symplicity device received CE mark approval in 2010.
Based on the clinical trial findings, Medtronic intends to form a panel of independent advisors of physicians and researchers who will be asked to make recommendations about the future of the global hypertension clinical trial program, as well as provide advice on continued physician and patient access to the Symplicity technology in countries with regulatory approvals. In the meantime, Medtronic will continue to make the device available to overseas patients in countries where the technology has been approved for use. The company also plans to continue the global post-market surveillance registry and renal denervation studies evaluating other non-hypertension indications. Follow-up for all patients randomized in the trial will continue as planned out to five years.
Though renal denervation is not a big part of Medtronic’s overall portfolio, the company’s brass was enthusiastic about its potential.
While “disappointed” with the results, Rick Kuntz, Medtronic’s chief medical officer said, “We believe this course of action is the most prudent and will help us thoroughly evaluate these findings and determine the appropriate next steps for renal denervation therapy.”
Medtronic paid $800 million in 2010 for a company called Ardian and its renal denervation technology.
Danielle Antalffy, with Leerink Research, said Medtronic’s news came as a surprise, following positive results from earlier trials. “The failed Symplicity HTN-3 trial could also have implications for the [renal denervation] market more broadly, bringing into question whether the catheter ablation approach is truly efficacious in reducing hypertension,” she wrote in a note to investors.
Covidien Bails, Others Maybe
Not long after Medtronic’s decision, Mansfield, Mass.-Covidien plc decided it was getting out of the renal denervation market, with officials citing “slower than expected development” of the sector. As a result, the company’s OneShot renal denervation program and related trial (called RAPID II) will end.
The device was approved in Europe in February 2012 but not in the United States. The decision resulted from Covidien’s “regular review of strategic programs and growth potential for various aspects of its product portfolio,” officials noted. The company also added that it “believes that the long-term hypertension market remains attractive and will continue to explore opportunities in this area.”
Covidien and Medtronic aren’t the only companies to turn their backs on renal denervation for hypertension.
In 2013, Natick, Mass.-based Boston Scientific bought a company called Vessix Vascular Inc., which developed a renal denervation system that had been approved for use in Europe and Australia. But it seems that Boston Scientific is planning to delay a U.S. trial of its Vessix product, at least for a while, according to Bloomberg news service. The trial was planned to start in July, but CEO Michael Mahoney said his company would “wait and see and learn more about the Medtronic trial results before we have broad discussion with the FDA (U.S. Food and Drug Administration) about what the trial design should be.”
Last year, St. Paul, Minn.-based St. Jude Medical Inc. announced that its EnligHTN renal denervation system safely and effectively lowered blood pressure at six months. In December, however, St. Jude discontinued the trial, citing recruitment challenges. The company said the move was not the result of a safety or efficacy issue with the device or study. On Jan. 22, during a conference call with reporters and analysts about the company’s financial results, President and CEO Daniel Stark said St. Jude was not abandoning the technology.
“We actually are very optimistic about the opportunity for renal denervation. Innovation is very often messy, and it takes patience and persistence,” Stark said. “We’re really looking forward to learning what we can from the Symplicity 3 [HTN-3] trial data and using that to help advance our program. But the Symplicity 3 announcement doesn’t change the fundamental reasons that we invested in the renal denervation space.”
There remains a “huge” unmet patient need, according to Stark.
“We don’t doubt that we’ll get a lot smarter from whatever data are presented as a result of the Symplicity 3 trial, and we’ll fully incorporate any of those lessons learned into our own program,” adding that the possibilities remain “warm” for renal denervation technology. Other companies “make decisions for different reasons and circumstances,” he noted, but St. Jude Medical can afford to wait.
“One of the benefits for us is that it’s less expensive for us to pursue our investment in renal denervation than with some other companies,” Stark explained. “We don’t have any acquisition expense that we run into the income statement. This is a homegrown, internal, very cost-effective program that leverages a tremendous amount of synergy from our 20 years of investment in the electrophysiology ablation space. We’re looking forward to [moving forward in] an area where we can really help patients.”
Other firms are charging ahead with the technology.
In January, privately held, Palo Alto, Calif.-based ReCor Medical received CE mark for the latest generation of its ultrasound-based renal denervation system. The first patients were treated with the system in December in Germany.
“Following the recent publication of negative results from one of the RDN (renal denervation) clinical trials, some competitors have announced that they are either delaying, reducing or abandoning efforts to commercialize their RF (radio frequency)-based RDN products. Having reviewed our own clinical results and spoken to clinicians who have collectively treated hundreds of patients with resistant hypertension using different RDN systems, ReCor is convinced that our product is well-differentiated from these RF-based approaches,” said Andrew M. Weiss, ReCor’s president and CEO.
What Happens Now?
Though companies may be taking time to reevaluate the market in light of Medtronic’s decision, the industry shouldn’t be quick to write off the technology. That would be “premature,” according toBernard Sweeney, senior vice president of medical devices for Reston, Va.-based Aptiv Solutions, a full-service international contract research organization that supports global clinical trials for biopharmaceutical and medical device companies.
“Unfortunately, at this stage, we still don’t have all the results. The first two studies produced fairly consistent but significant results. From that point of view, one would naturally assume that the third in the series would produce similar results,” Sweeney told Medical Product Oursourcing. “It didn’t, but we can still learn from that. Some companies are saying, ‘Let’s have a look at what Medtronic has done. If there’s something to learn, let’s do it now and reduce our risk.’ For other companies, they probably have thoughts and ideas that aren’t changed by this decision, because they’re looking at the clinical problem from another angle or approach it differently.”
Large companies have had products in the European market for a number of years and there’s data about how these products have performed on a real-time basis, which can’t be ignored, he cautioned.
Sweeney noted that once full trial results are available from Medtronic, companies can make critical decisions about their own trial design as they pursue renal denervation device solutions.
“Perhaps by changing the way they look at the study, by looking at different designs, they could possibly give themselves more flexibility and ability to work with the study, then alter it depending on what they find,” he said. “There are more studies that have been completed—perhaps smaller—but they have produced consistently good results. Perhaps the opportunity needs to be evaluated with more research, with multiple etiologies. If the studies are structured with an adaptive design, it gives [companies] more flexibility to look at the individual patient.”
Adaptive clinical trials use interim data analysis to re-assess trial methodology and make alterations where necessary during the trial. According to Aptiv officials, the use of adaptive trial design for medical devices is growing, as is support from the FDA. (Editor’s note: An upcoming issue of MPO will explore adaptive clinical trial design in greater detail.)
“I would be very surprised if renal denervation disappears, because there is significant evidence that this technology can affect hypertension safely,” Sweeney said.
In fact, many start-ups jumped on the renal denervation bandwagon only to be snatched up (often for hundreds of millions of dollars) by the likes of Medtronic Inc. and Boston Scientific Corp.
Similar to angioplasty, renal denervation involves snaking a catheter through the femoral artery up to the renal arteries, where it uses heat to deactivate the renal nerves (in the kidneys) which, in theory, lowers blood pressure. Hypertension is associated with an overactive sympathetic drive and renal denervation is the ablation of the renal nerves to stop the “talk” between the kidneys and the brain, thus reducing the sympathetic drive. Congestive heart failure, left ventricular hypertrophy, atrial fibrillation, obstructive sleep apnea, and insulin-resistant type 2 diabetes also are associated with an overactive sympathetic drive. Current clinical trials are researching the effect of renal denervation in these clinical conditions as well, according to RDNworld.com.
The prospects—according to industry number crunchers—for steadily increasing sales in the renal denervation market for hypertension have seemed relatively certain. As recently as December 2013, a report from industry research firm Global Data predicted that the global renal denervation market would grow from $15.5 million in 2012 to $171.7 million by 2019 at a compound annual growth rate of 41 percent, driven by the technology’s approval in major countries, including the United States, by the end of 2019.
What a difference a month can make.
Medtronic Puts on the Brakes
On Jan. 9, Medtronic announced that it would discontinue its third renal denervation study, ending a large U.S. trial for its
Symplicity renal denervation system. The trial, Symplicity HTN-3, met its primary safety endpoint related to the incidence of major adverse events, but it did not meet its primary efficacy endpoint of a change in office blood pressure from baseline to six months. The company claims it was the most rigorous renal denervation study to date.
The Symplicity HTN-1 and HTN-2 trials also demonstrated a good safety profile for catheter-based renal denervation.
While certainly a blow for the Minneapolis, Minn.-based medtech behemoth, the news has a wider industry impact and puts in doubt the future of renal denervation, and what some analysts predicted ultimately could become a billion-dollar worldwide market. According to Medtronic, roughly 1.2 billion people worldwide suffer from high blood pressure and about one-third don’t respond to medication.
In addition to ending the trial, which involved 535 patients at 87 medical centers throughout the United States, Medtronic also stopped recruiting patients for clinical trials in Japan and India. In Europe, the Symplicity device received CE mark approval in 2010.
Based on the clinical trial findings, Medtronic intends to form a panel of independent advisors of physicians and researchers who will be asked to make recommendations about the future of the global hypertension clinical trial program, as well as provide advice on continued physician and patient access to the Symplicity technology in countries with regulatory approvals. In the meantime, Medtronic will continue to make the device available to overseas patients in countries where the technology has been approved for use. The company also plans to continue the global post-market surveillance registry and renal denervation studies evaluating other non-hypertension indications. Follow-up for all patients randomized in the trial will continue as planned out to five years.
Though renal denervation is not a big part of Medtronic’s overall portfolio, the company’s brass was enthusiastic about its potential.
While “disappointed” with the results, Rick Kuntz, Medtronic’s chief medical officer said, “We believe this course of action is the most prudent and will help us thoroughly evaluate these findings and determine the appropriate next steps for renal denervation therapy.”
Medtronic paid $800 million in 2010 for a company called Ardian and its renal denervation technology.
Danielle Antalffy, with Leerink Research, said Medtronic’s news came as a surprise, following positive results from earlier trials. “The failed Symplicity HTN-3 trial could also have implications for the [renal denervation] market more broadly, bringing into question whether the catheter ablation approach is truly efficacious in reducing hypertension,” she wrote in a note to investors.
Covidien Bails, Others Maybe
Not long after Medtronic’s decision, Mansfield, Mass.-Covidien plc decided it was getting out of the renal denervation market, with officials citing “slower than expected development” of the sector. As a result, the company’s OneShot renal denervation program and related trial (called RAPID II) will end.
The device was approved in Europe in February 2012 but not in the United States. The decision resulted from Covidien’s “regular review of strategic programs and growth potential for various aspects of its product portfolio,” officials noted. The company also added that it “believes that the long-term hypertension market remains attractive and will continue to explore opportunities in this area.”
Covidien and Medtronic aren’t the only companies to turn their backs on renal denervation for hypertension.
In 2013, Natick, Mass.-based Boston Scientific bought a company called Vessix Vascular Inc., which developed a renal denervation system that had been approved for use in Europe and Australia. But it seems that Boston Scientific is planning to delay a U.S. trial of its Vessix product, at least for a while, according to Bloomberg news service. The trial was planned to start in July, but CEO Michael Mahoney said his company would “wait and see and learn more about the Medtronic trial results before we have broad discussion with the FDA (U.S. Food and Drug Administration) about what the trial design should be.”
Last year, St. Paul, Minn.-based St. Jude Medical Inc. announced that its EnligHTN renal denervation system safely and effectively lowered blood pressure at six months. In December, however, St. Jude discontinued the trial, citing recruitment challenges. The company said the move was not the result of a safety or efficacy issue with the device or study. On Jan. 22, during a conference call with reporters and analysts about the company’s financial results, President and CEO Daniel Stark said St. Jude was not abandoning the technology.
“We actually are very optimistic about the opportunity for renal denervation. Innovation is very often messy, and it takes patience and persistence,” Stark said. “We’re really looking forward to learning what we can from the Symplicity 3 [HTN-3] trial data and using that to help advance our program. But the Symplicity 3 announcement doesn’t change the fundamental reasons that we invested in the renal denervation space.”
There remains a “huge” unmet patient need, according to Stark.
“We don’t doubt that we’ll get a lot smarter from whatever data are presented as a result of the Symplicity 3 trial, and we’ll fully incorporate any of those lessons learned into our own program,” adding that the possibilities remain “warm” for renal denervation technology. Other companies “make decisions for different reasons and circumstances,” he noted, but St. Jude Medical can afford to wait.
“One of the benefits for us is that it’s less expensive for us to pursue our investment in renal denervation than with some other companies,” Stark explained. “We don’t have any acquisition expense that we run into the income statement. This is a homegrown, internal, very cost-effective program that leverages a tremendous amount of synergy from our 20 years of investment in the electrophysiology ablation space. We’re looking forward to [moving forward in] an area where we can really help patients.”
Other firms are charging ahead with the technology.
In January, privately held, Palo Alto, Calif.-based ReCor Medical received CE mark for the latest generation of its ultrasound-based renal denervation system. The first patients were treated with the system in December in Germany.
“Following the recent publication of negative results from one of the RDN (renal denervation) clinical trials, some competitors have announced that they are either delaying, reducing or abandoning efforts to commercialize their RF (radio frequency)-based RDN products. Having reviewed our own clinical results and spoken to clinicians who have collectively treated hundreds of patients with resistant hypertension using different RDN systems, ReCor is convinced that our product is well-differentiated from these RF-based approaches,” said Andrew M. Weiss, ReCor’s president and CEO.
What Happens Now?
Though companies may be taking time to reevaluate the market in light of Medtronic’s decision, the industry shouldn’t be quick to write off the technology. That would be “premature,” according toBernard Sweeney, senior vice president of medical devices for Reston, Va.-based Aptiv Solutions, a full-service international contract research organization that supports global clinical trials for biopharmaceutical and medical device companies.
“Unfortunately, at this stage, we still don’t have all the results. The first two studies produced fairly consistent but significant results. From that point of view, one would naturally assume that the third in the series would produce similar results,” Sweeney told Medical Product Oursourcing. “It didn’t, but we can still learn from that. Some companies are saying, ‘Let’s have a look at what Medtronic has done. If there’s something to learn, let’s do it now and reduce our risk.’ For other companies, they probably have thoughts and ideas that aren’t changed by this decision, because they’re looking at the clinical problem from another angle or approach it differently.”
Large companies have had products in the European market for a number of years and there’s data about how these products have performed on a real-time basis, which can’t be ignored, he cautioned.
Sweeney noted that once full trial results are available from Medtronic, companies can make critical decisions about their own trial design as they pursue renal denervation device solutions.
“Perhaps by changing the way they look at the study, by looking at different designs, they could possibly give themselves more flexibility and ability to work with the study, then alter it depending on what they find,” he said. “There are more studies that have been completed—perhaps smaller—but they have produced consistently good results. Perhaps the opportunity needs to be evaluated with more research, with multiple etiologies. If the studies are structured with an adaptive design, it gives [companies] more flexibility to look at the individual patient.”
Adaptive clinical trials use interim data analysis to re-assess trial methodology and make alterations where necessary during the trial. According to Aptiv officials, the use of adaptive trial design for medical devices is growing, as is support from the FDA. (Editor’s note: An upcoming issue of MPO will explore adaptive clinical trial design in greater detail.)
“I would be very surprised if renal denervation disappears, because there is significant evidence that this technology can affect hypertension safely,” Sweeney said.