UC Davis Health System04.14.16
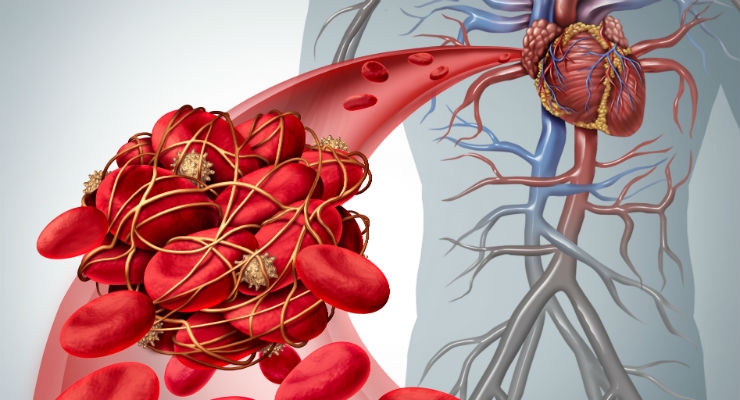
Devices intended to stop potentially deadly blood clots from reaching the lungs can help a small portion of the patients who receive them but can also increase the risk of additional clots, researchers at UC Davis Health System have found.
Published online in the journal Circulation, the study is the first to distinguish patients who should receive the device, known as an inferior vena cava (IVC) filter, from those who should instead be treated only with standard anticoagulation medications like heparin or warfarin.
“Decisions about the use of IVC filters have so far not been driven by good science, primarily because there have been only two very small clinical trials that studied them,” said lead author Richard White, chief of general medicine and medical director of the anticoagulation service at UC Davis. “Our results will help physicians know when a filter may be helpful and when it should not be considered.”
Shaped like small wire traps, IVC filters are inserted into the major vein in the abdomen just below the kidneys to block or break up clots traveling from the lower to the upper body. Some physicians recommend them for patients with leg or lung blood clots. White and others, however, have suspected that the presence of blood clots alone wasn’t enough to warrant use of the filters.
For the study, White and his team evaluated one-year outcomes, including deaths and new blood-clot occurrences, in about 85,000 adult patients hospitalized in California between 2005 through 2010 for acute pulmonary embolism (a blood clot in a lung artery) or acute deep-vein thrombosis (a blood clot in a leg vein). Overall, 11 percent of patients in the study received IVC filters as part of their blood clot treatments.
Patients included in the analysis were divided into three groups: those who could be treated with standard anticoagulant therapy, those who had active bleeding and could not be treated with anticoagulants, and those who had very recent or emergency surgery and needed to be off anticoagulants for a short time.
There were three standout outcomes:
For the 1,400 patients in the study who either recently had surgery or required surgery, use of a filter provided no benefits, but also no harms.
“It’s likely that these patients had anticoagulants withheld for just a short time after surgery,” White said. “Unless anticoagulation therapy can’t be restarted after surgery, a filter isn’t likely to be beneficial.”
White added that the study results support current American College of Chest Physicians (ACCP) clinical guidelines, which recommend IVC filters only for patients with newly diagnosed blood clots who cannot be treated with standard anticoagulants.
“We are confident in confirming the ACCP’s guidelines for acute blood clot treatment,” said White. “Our results should reduce indiscriminate use of the filters and help physicians provide informed and safe options for patients.”
White’s co-authors were Ann Brunson, Patrick Romano, Zhongmin Li and Ted Wun of UC Davis. Their work was supported by the Hibbard E. Williams Endowment at UC Davis.
A copy of the study, titled “Outcomes after Vena Cava Filter Use in Non-cancer Patients with Acute Venous Thromboembolism: A Population-Based Study,” can be requested by emailing bridgette.mcneill@heart.org.
Published online in the journal Circulation, the study is the first to distinguish patients who should receive the device, known as an inferior vena cava (IVC) filter, from those who should instead be treated only with standard anticoagulation medications like heparin or warfarin.
“Decisions about the use of IVC filters have so far not been driven by good science, primarily because there have been only two very small clinical trials that studied them,” said lead author Richard White, chief of general medicine and medical director of the anticoagulation service at UC Davis. “Our results will help physicians know when a filter may be helpful and when it should not be considered.”
Shaped like small wire traps, IVC filters are inserted into the major vein in the abdomen just below the kidneys to block or break up clots traveling from the lower to the upper body. Some physicians recommend them for patients with leg or lung blood clots. White and others, however, have suspected that the presence of blood clots alone wasn’t enough to warrant use of the filters.
For the study, White and his team evaluated one-year outcomes, including deaths and new blood-clot occurrences, in about 85,000 adult patients hospitalized in California between 2005 through 2010 for acute pulmonary embolism (a blood clot in a lung artery) or acute deep-vein thrombosis (a blood clot in a leg vein). Overall, 11 percent of patients in the study received IVC filters as part of their blood clot treatments.
Patients included in the analysis were divided into three groups: those who could be treated with standard anticoagulant therapy, those who had active bleeding and could not be treated with anticoagulants, and those who had very recent or emergency surgery and needed to be off anticoagulants for a short time.
There were three standout outcomes:
- IVC filters reduced 30- and 90-day mortality by 30 percent for the small number of patients in the study (3.5 percent) who had active bleeding. However, the filters also increased the risk of new leg blood clots for these patients by 135 percent.
- Use of an IVC filter did not benefit patients who could receive anticoagulation treatment and, compared to those who did not receive filters, it increased the risk of new blood clots forming in the legs by 50 percent.
- IVC filters had no effect on the incidence of subsequent pulmonary embolism, one of the primary reasons why physicians tend to use them.
For the 1,400 patients in the study who either recently had surgery or required surgery, use of a filter provided no benefits, but also no harms.
“It’s likely that these patients had anticoagulants withheld for just a short time after surgery,” White said. “Unless anticoagulation therapy can’t be restarted after surgery, a filter isn’t likely to be beneficial.”
White added that the study results support current American College of Chest Physicians (ACCP) clinical guidelines, which recommend IVC filters only for patients with newly diagnosed blood clots who cannot be treated with standard anticoagulants.
“We are confident in confirming the ACCP’s guidelines for acute blood clot treatment,” said White. “Our results should reduce indiscriminate use of the filters and help physicians provide informed and safe options for patients.”
White’s co-authors were Ann Brunson, Patrick Romano, Zhongmin Li and Ted Wun of UC Davis. Their work was supported by the Hibbard E. Williams Endowment at UC Davis.
A copy of the study, titled “Outcomes after Vena Cava Filter Use in Non-cancer Patients with Acute Venous Thromboembolism: A Population-Based Study,” can be requested by emailing bridgette.mcneill@heart.org.