Sam Brusco, Associate Editor05.02.22
Peripheral nerve stimulation (PNS) was first used in Philadelphia in the 1960s to treat head and neck pain. Back then, it was an open surgery. The surgeon dissected tissue to visualize the nerve and insert the neurostimulating lead. It was later modified to use a transposed fascial graft between the nerve and lead. This eventually lost favor because it was too complex and had too many adverse effects.
The technique has been used in increasingly less invasive forms to treat disease, including pain, for decades since. The technique fundamentally changed in 1999 with the publishing of a study that used percutaneous leads originally designed for the spinal cord to treat occipital neuropathic headaches. Unfortunately, in 2011 a randomized multicenter prospective study to assess PNS’ safety and efficacy failed to meet its primary endpoint. However, the revealed adverse lead erosion and migration events formed further basis to perfect the technique.
Technological innovation has transformed PNS into a more viable chronic pain therapy, and interest continues to increase as patients seek out opioid alternatives to manage their suffering. The first clinical study for a minimally invasive PNS device came via a U.S. Food and Drug Administration (FDA) Investigational Device Exemption (IDE) study using a small implantable tined lead and external peripheral nerve generator. The device was called StimRouter, manufactured by Valencia, Calif.-based Bioness (now part of Durham, N.C.-based active healing firm Bioventus), which was founded by physicist, inventor, entrepreneur, and philanthropist Alfred Mann. StimRouter won FDA approval for PNS to treat chronic, intractable pain in the trunk and limbs in 2015.
The PNS market, though small, is quickly evolving. The latest generation of StimRouter—which features a smartphone application to manage therapy and an upgraded external electric field conductor—earned FDA 510(k) clearance on March 1. On March 28, Cleveland, Ohio-based SPR Therapeutics’ Sprint PNS for both acute and chronic pain therapy won Cleveland Inno’s inaugural “Inno Madness” four-month competition between 16 promising startups. The company also received $37 million in funding last fall. On April 19, Pompano Beach, Fla.-based neuromodulation company Stimwave announced initiation of its level-1 FREEDOM clinical trial series to evaluate its Freedom PNS for chronic knee pain, aiming to reduce pain by 50 percent or more.
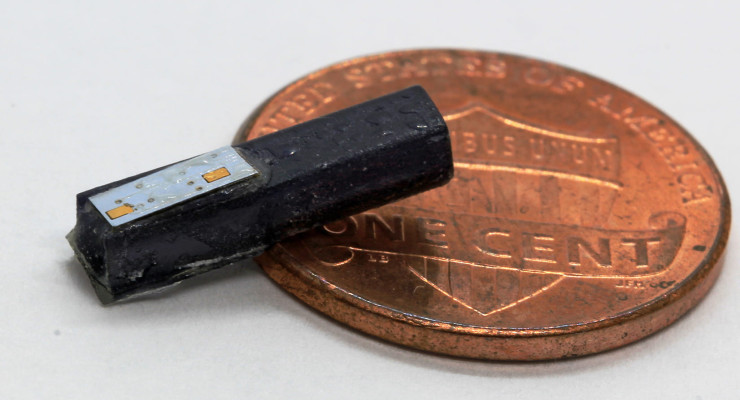
Houston’s Rice University believes PNS technology could be reduced to about the size of a grain of rice.
Rice engineers and a host of Texas Medical Center institutions published proof-of-concept results in Nature Biomedical Engineering on March 31 from a years-long program to build tiny, wireless devices to treat neurological ailments or block pain. The star of the study, the 0.8 square-millimeter MagnetoElectric Bio ImplanT—ME-BIT, for short—is delivered to the intended stimulation target through a percutaneous catheter. ME-BIT doesn’t need a battery, instead drawing power and programming from a low-powered, ex vivo magnetic transmitter worn close to the body.
ME-BIT’s transmitter was successfully tested on animal models, where it was able to charge and communicate with implants several centimeters below the skin. The researchers believe it could replace more invasive units now treating Parkinson’s, epilepsy, chronic pain, hearing loss, and paralysis.
“Because the devices are so small, we can use blood vessels as a highway system to reach targets that are difficult to get to with traditional surgery,” Rice Neuroengineering Initiative researcher and co-team leader Jacob Robinson told the press. “We’re delivering them using the same catheters you would use for an endovascular procedure, but we would leave the device outside the vessel and place a guidewire into the bloodstream as the stimulating electrode, which could be held in place with a stent.”
The implant’s wireless power is achieved via a strip of magnetoelectric film that converts magnetic energy into electrical power. Its onboard capacitor stores some of the power, and a so-called “system-on-a-chip” microprocessor translates magnetic field modulations into data. A 3D-printed capsule holds all the components together, then the capsule is further encased in epoxy.
Body tissues easily tolerate the approximately 1 milliTesla magnetic field generated by the transmitter, according to the researchers. They estimated the current implant could generate four milliwatts of power at maximum, which is sufficient for various neurostimulation therapies.
“One of the nice things is that all the nerves in our bodies require oxygen and nutrients, so that means there’s a blood vessel within a few hundred microns of all the nerves,” Robinson said. “It’s just a matter of tracing the right blood vessels to reach the targets. With a combination of imaging and anatomy, we can be pretty confident about where we place the electrodes.”
The research hints endovascular bioelectronics like ME-BIT could provide a foundation for a bevy of low-risk, precise therapies. Electrodes in the bloodstream might also allow for real-time biochemical, pH, and blood-oxygen level sensing for diagnostics or to support other medical devices.
Eventually, the team hopes to employ multiple implants and communicate with them at the same time.
“That way we could have a distributed network at multiple sites,” he said. “Other things we’re looking to add are sensing, recording, and back-channel communications so we can use the implants to both record and stimulate activity as part of a closed system.”
The technique has been used in increasingly less invasive forms to treat disease, including pain, for decades since. The technique fundamentally changed in 1999 with the publishing of a study that used percutaneous leads originally designed for the spinal cord to treat occipital neuropathic headaches. Unfortunately, in 2011 a randomized multicenter prospective study to assess PNS’ safety and efficacy failed to meet its primary endpoint. However, the revealed adverse lead erosion and migration events formed further basis to perfect the technique.
Technological innovation has transformed PNS into a more viable chronic pain therapy, and interest continues to increase as patients seek out opioid alternatives to manage their suffering. The first clinical study for a minimally invasive PNS device came via a U.S. Food and Drug Administration (FDA) Investigational Device Exemption (IDE) study using a small implantable tined lead and external peripheral nerve generator. The device was called StimRouter, manufactured by Valencia, Calif.-based Bioness (now part of Durham, N.C.-based active healing firm Bioventus), which was founded by physicist, inventor, entrepreneur, and philanthropist Alfred Mann. StimRouter won FDA approval for PNS to treat chronic, intractable pain in the trunk and limbs in 2015.
The PNS market, though small, is quickly evolving. The latest generation of StimRouter—which features a smartphone application to manage therapy and an upgraded external electric field conductor—earned FDA 510(k) clearance on March 1. On March 28, Cleveland, Ohio-based SPR Therapeutics’ Sprint PNS for both acute and chronic pain therapy won Cleveland Inno’s inaugural “Inno Madness” four-month competition between 16 promising startups. The company also received $37 million in funding last fall. On April 19, Pompano Beach, Fla.-based neuromodulation company Stimwave announced initiation of its level-1 FREEDOM clinical trial series to evaluate its Freedom PNS for chronic knee pain, aiming to reduce pain by 50 percent or more.
Houston’s Rice University believes PNS technology could be reduced to about the size of a grain of rice.
Rice engineers and a host of Texas Medical Center institutions published proof-of-concept results in Nature Biomedical Engineering on March 31 from a years-long program to build tiny, wireless devices to treat neurological ailments or block pain. The star of the study, the 0.8 square-millimeter MagnetoElectric Bio ImplanT—ME-BIT, for short—is delivered to the intended stimulation target through a percutaneous catheter. ME-BIT doesn’t need a battery, instead drawing power and programming from a low-powered, ex vivo magnetic transmitter worn close to the body.
ME-BIT’s transmitter was successfully tested on animal models, where it was able to charge and communicate with implants several centimeters below the skin. The researchers believe it could replace more invasive units now treating Parkinson’s, epilepsy, chronic pain, hearing loss, and paralysis.
“Because the devices are so small, we can use blood vessels as a highway system to reach targets that are difficult to get to with traditional surgery,” Rice Neuroengineering Initiative researcher and co-team leader Jacob Robinson told the press. “We’re delivering them using the same catheters you would use for an endovascular procedure, but we would leave the device outside the vessel and place a guidewire into the bloodstream as the stimulating electrode, which could be held in place with a stent.”
The implant’s wireless power is achieved via a strip of magnetoelectric film that converts magnetic energy into electrical power. Its onboard capacitor stores some of the power, and a so-called “system-on-a-chip” microprocessor translates magnetic field modulations into data. A 3D-printed capsule holds all the components together, then the capsule is further encased in epoxy.
Body tissues easily tolerate the approximately 1 milliTesla magnetic field generated by the transmitter, according to the researchers. They estimated the current implant could generate four milliwatts of power at maximum, which is sufficient for various neurostimulation therapies.
“One of the nice things is that all the nerves in our bodies require oxygen and nutrients, so that means there’s a blood vessel within a few hundred microns of all the nerves,” Robinson said. “It’s just a matter of tracing the right blood vessels to reach the targets. With a combination of imaging and anatomy, we can be pretty confident about where we place the electrodes.”
The research hints endovascular bioelectronics like ME-BIT could provide a foundation for a bevy of low-risk, precise therapies. Electrodes in the bloodstream might also allow for real-time biochemical, pH, and blood-oxygen level sensing for diagnostics or to support other medical devices.
Eventually, the team hopes to employ multiple implants and communicate with them at the same time.
“That way we could have a distributed network at multiple sites,” he said. “Other things we’re looking to add are sensing, recording, and back-channel communications so we can use the implants to both record and stimulate activity as part of a closed system.”
