Chris Oleksy, Oleksy Enterprises and Next Life Medical04.06.16
Have you ever driven from San Diego to New York City without the help of a GPS, MapQuest, or even an atlas? Probably not. Believe it or not, many of us remember the days when you would call the American Automobile Association (AAA) and tell them your point of origin and destination and they would put together a printed map book for you. And those same readers (and author) remember when you had to make a phone call to get the time and temperature. There was no access to an atomic clock, internet, or GPS to simplify your journey as there is today.
In my last article that appeared in the March issue of MPO, Today’s Healthcare Tug-of-War: The Supply Chain vs. the Care Chain, I introduced readers to the difference between a supply chain and a care chain and the frequent tug-of-war between the two. I suggested that the patient should be the point of origin, or starting point, not the ending point, or destination on our way to taking cost out of our chains.
Throughout my career, I have configured hundreds of care chains on the way to saving hundreds of millions of dollars, but have always kept the patient in my line of sight. Those that know me personally know that I am 100 percent in favor of saving money and love to clip coupons. But I won’t use a coupon just to use a coupon. If I don’t want a pizza tonight, and the coupon is expiring, so be it. There needs to be a means (the patient) to an end (lower cost delivery mechanisms without compromising the patient). And it can be done.
In this month’s column, my goal is to help you understand how to accomplish a means to an end by using the concept of color-coded thread mapping. Color-coded thread mapping is a critical portion of the Oleksy Enterprises OE-Tier5 model that will be explained in my next column. Color-coded thread mapping is the concept of developing a route between point B (the patient) and point A (the manufacturer). Notice I didn’t say point A to point B. I said point B to point A. This ensures we keep the patient as the point of origin, and not the final destination; a subtle but extremely important enunciation.
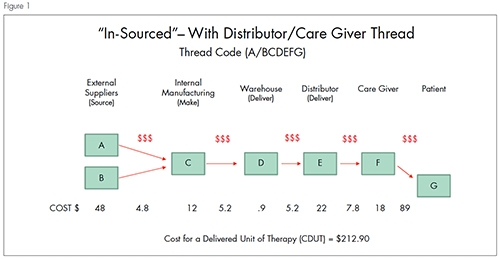
There are many examples of color-coded mapping and it can be applied in many different situations. But first, the concept of drawing thread maps must be understood. Figure 1 demonstrates a care chain thread scenario typical of a product as it evolves. This diagram shows outside suppliers (A-B) supplying plant C and then onto the warehouse and so on. The $ signs between the boxes reflect hand-offs, which indicate cost add. These do not imply they are non-value-added steps, but are present to signify cost being added as the product is being moved through the care chain. The care chain code assigned to this product thread is A/BCDEFG.
Even though the drawing is a synchronous “push” from left to right, the thinking needs to be a “pull” process from right to left. Patient needs care; care giver provides care; care giver needs product; and so on.
Once we have the thread mapped, we can calculate the cost of a delivered unit of therapy (CDUT), which is the cost of the product plus the logistics cost plus the therapy delivery cost throughout the care chain. In this hypothetical example, the CDUT is $212.90. This example is completely hypothetical in order create a base line for this thread. You should create a baseline or starting point that is as accurate as you can get; this in itself is an eye-opening exercise.
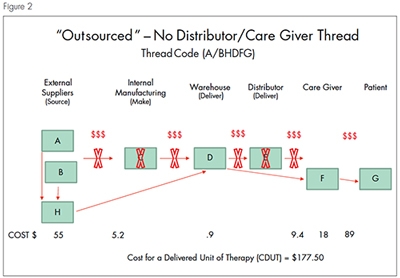
Once we have the thread mapped, we can now assess other scenarios such as upper management asking us to evaluate out-sourcing this product and eliminating the distributor. Therefore, I have mapped out the new scenario in Figure 2. Figure 2 reflects sending the raw materials from suppliers A and B to supplier H. Then, H ships a finished product to a warehouse D and so on. The resulting care chain is A/BHDFG. The CDUT drops to $177.50, or a savings of 16.6 percent.
It’s arguable that this is a slam dunk—but that would be a trap. There are many attributes that need to be considered during this exercise, including (not a comprehensive list):
In over 35 years of experience across the medical device industry, with multiple OEMs and virtually thousands of care chains, I have come to realize that less than 10 percent of care chains are actually mapped out, and about 5 percent actually stay intact after the exercise because there are always opportunities to improve. And where there are no opportunities for improvement, after mapping, you will at least have identified the “why.”
Being a supply chain-wired person, I love Amazon and direct ship models. But even with Amazon, there is a time that is appropriate for me to use it, and a time it is not. It is a case-by-case scenario, and requires my actions to be aligned with a given outcome—such as the means to an end mentioned previously. Just because I can use Amazon doesn’t always mean I should.
My next article will be about the OE-Tier5 models I have been perfecting for many years to help guide the alignment of our actions to ensure they support our direction. Misguided actions are like getting out of the car on your Jurassic Park ride—not a good idea!
As I said in March MPO, we live in the healthcare space. We’re not buying hammers for a home improvement store; we’re taking care of people. And maybe we should even be a bit more selfish. Don’t we owe it to ourselves and our families to map out our care chains for our own good? Personally, I want the best possible care I can get, with the best possible outcome and value. In the absence of mapping, we end up with what Zig Ziglar used to say about cutting the ends off hams—it’s done that way because “grandma always did it that way.”
Since AAA is not in the profession of mapping your care chain, and a GPS or atomic clock won’t help, you had better get to work.
Chris Oleksy is founder and CEO of Oleksy Enterprises and Next Life Medical. He can be reached at chris@oleksyenterprises.com.
In my last article that appeared in the March issue of MPO, Today’s Healthcare Tug-of-War: The Supply Chain vs. the Care Chain, I introduced readers to the difference between a supply chain and a care chain and the frequent tug-of-war between the two. I suggested that the patient should be the point of origin, or starting point, not the ending point, or destination on our way to taking cost out of our chains.
Throughout my career, I have configured hundreds of care chains on the way to saving hundreds of millions of dollars, but have always kept the patient in my line of sight. Those that know me personally know that I am 100 percent in favor of saving money and love to clip coupons. But I won’t use a coupon just to use a coupon. If I don’t want a pizza tonight, and the coupon is expiring, so be it. There needs to be a means (the patient) to an end (lower cost delivery mechanisms without compromising the patient). And it can be done.
In this month’s column, my goal is to help you understand how to accomplish a means to an end by using the concept of color-coded thread mapping. Color-coded thread mapping is a critical portion of the Oleksy Enterprises OE-Tier5 model that will be explained in my next column. Color-coded thread mapping is the concept of developing a route between point B (the patient) and point A (the manufacturer). Notice I didn’t say point A to point B. I said point B to point A. This ensures we keep the patient as the point of origin, and not the final destination; a subtle but extremely important enunciation.
There are many examples of color-coded mapping and it can be applied in many different situations. But first, the concept of drawing thread maps must be understood. Figure 1 demonstrates a care chain thread scenario typical of a product as it evolves. This diagram shows outside suppliers (A-B) supplying plant C and then onto the warehouse and so on. The $ signs between the boxes reflect hand-offs, which indicate cost add. These do not imply they are non-value-added steps, but are present to signify cost being added as the product is being moved through the care chain. The care chain code assigned to this product thread is A/BCDEFG.
Even though the drawing is a synchronous “push” from left to right, the thinking needs to be a “pull” process from right to left. Patient needs care; care giver provides care; care giver needs product; and so on.
Once we have the thread mapped, we can calculate the cost of a delivered unit of therapy (CDUT), which is the cost of the product plus the logistics cost plus the therapy delivery cost throughout the care chain. In this hypothetical example, the CDUT is $212.90. This example is completely hypothetical in order create a base line for this thread. You should create a baseline or starting point that is as accurate as you can get; this in itself is an eye-opening exercise.
Once we have the thread mapped, we can now assess other scenarios such as upper management asking us to evaluate out-sourcing this product and eliminating the distributor. Therefore, I have mapped out the new scenario in Figure 2. Figure 2 reflects sending the raw materials from suppliers A and B to supplier H. Then, H ships a finished product to a warehouse D and so on. The resulting care chain is A/BHDFG. The CDUT drops to $177.50, or a savings of 16.6 percent.
It’s arguable that this is a slam dunk—but that would be a trap. There are many attributes that need to be considered during this exercise, including (not a comprehensive list):
- Is the quality of the product coming from supplier H as good as or better than that being made internally in plant C?
- Is supplier H reputable and cognizant of the needs of the patient? and
- There is an assumption in Figure 2 that the distributor is not needed. Has this been truly vetted out? Oftentimes, a hybrid approach is logical where both options to ship direct from the warehouse and from the distributor are needed.
In over 35 years of experience across the medical device industry, with multiple OEMs and virtually thousands of care chains, I have come to realize that less than 10 percent of care chains are actually mapped out, and about 5 percent actually stay intact after the exercise because there are always opportunities to improve. And where there are no opportunities for improvement, after mapping, you will at least have identified the “why.”
Being a supply chain-wired person, I love Amazon and direct ship models. But even with Amazon, there is a time that is appropriate for me to use it, and a time it is not. It is a case-by-case scenario, and requires my actions to be aligned with a given outcome—such as the means to an end mentioned previously. Just because I can use Amazon doesn’t always mean I should.
My next article will be about the OE-Tier5 models I have been perfecting for many years to help guide the alignment of our actions to ensure they support our direction. Misguided actions are like getting out of the car on your Jurassic Park ride—not a good idea!
As I said in March MPO, we live in the healthcare space. We’re not buying hammers for a home improvement store; we’re taking care of people. And maybe we should even be a bit more selfish. Don’t we owe it to ourselves and our families to map out our care chains for our own good? Personally, I want the best possible care I can get, with the best possible outcome and value. In the absence of mapping, we end up with what Zig Ziglar used to say about cutting the ends off hams—it’s done that way because “grandma always did it that way.”
Since AAA is not in the profession of mapping your care chain, and a GPS or atomic clock won’t help, you had better get to work.
Chris Oleksy is founder and CEO of Oleksy Enterprises and Next Life Medical. He can be reached at chris@oleksyenterprises.com.